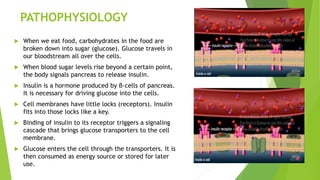
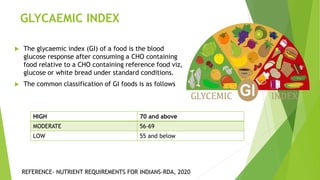
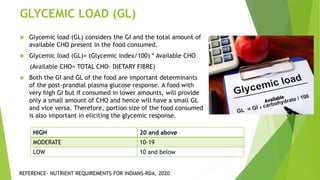
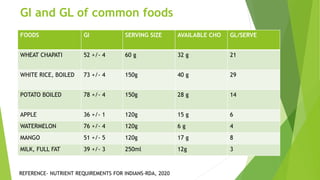
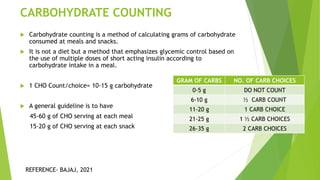
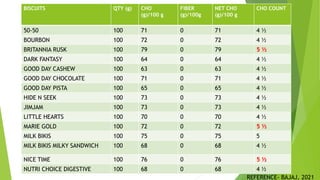
This document provides information on type 2 diabetes mellitus. It begins with an introduction defining diabetes and describing the pathogenesis of type 2 diabetes. It then discusses the pathophysiology in detail, explaining how insulin resistance and relative insulin deficiency lead to hyperglycemia. The etiology, symptoms, acute and chronic complications, diagnosis and management of type 2 diabetes are also summarized. Management includes dietary recommendations focusing on macronutrient distribution using strategies like glycemic index, glycemic load and carbohydrate counting to improve glycemic control.


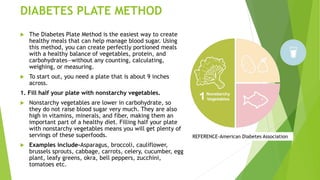
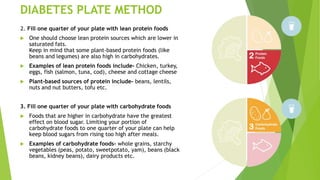
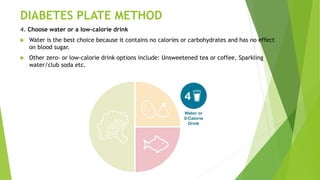
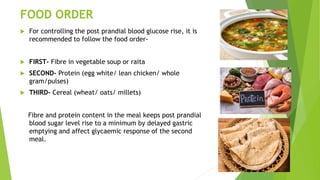

















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















