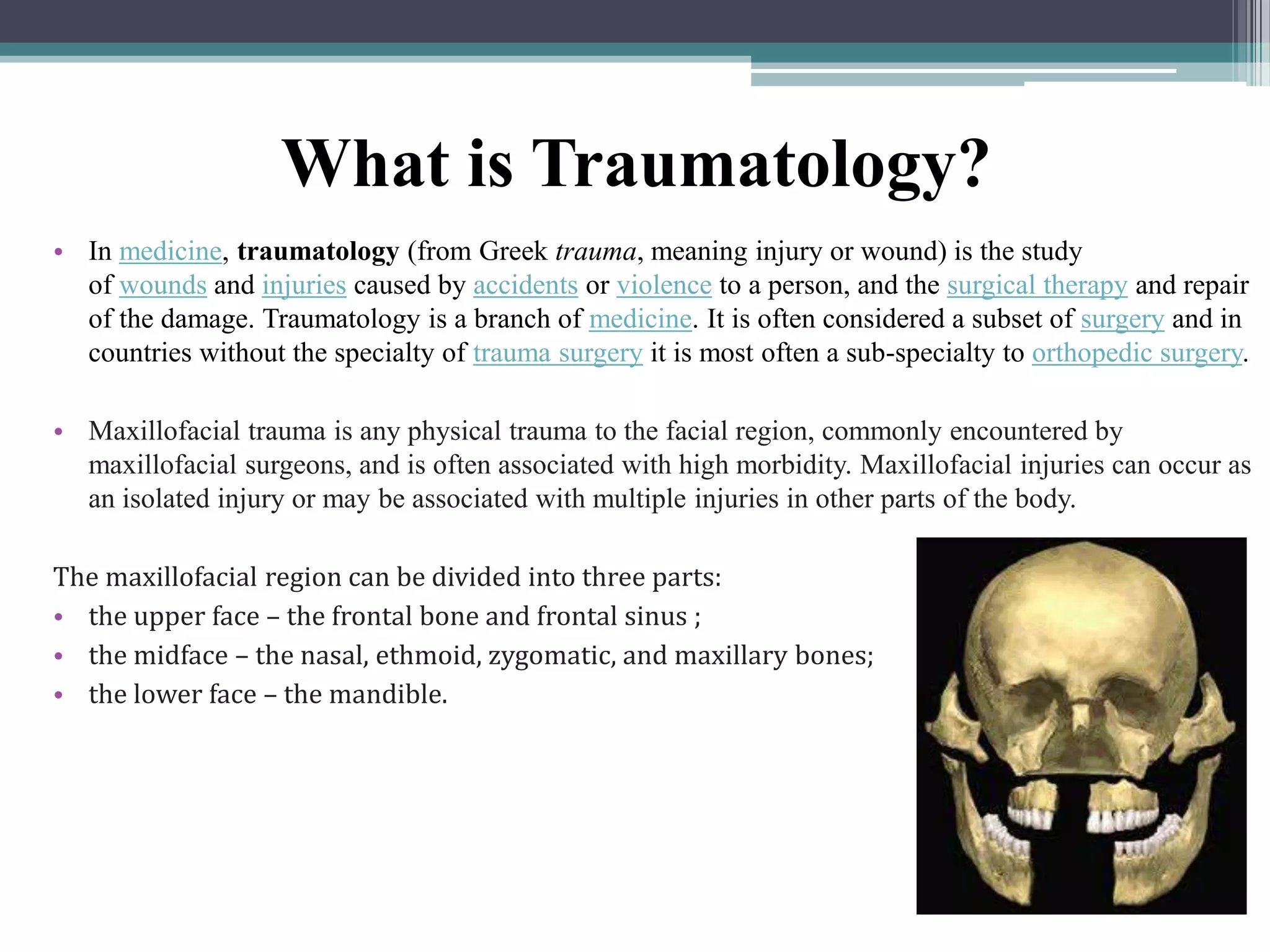
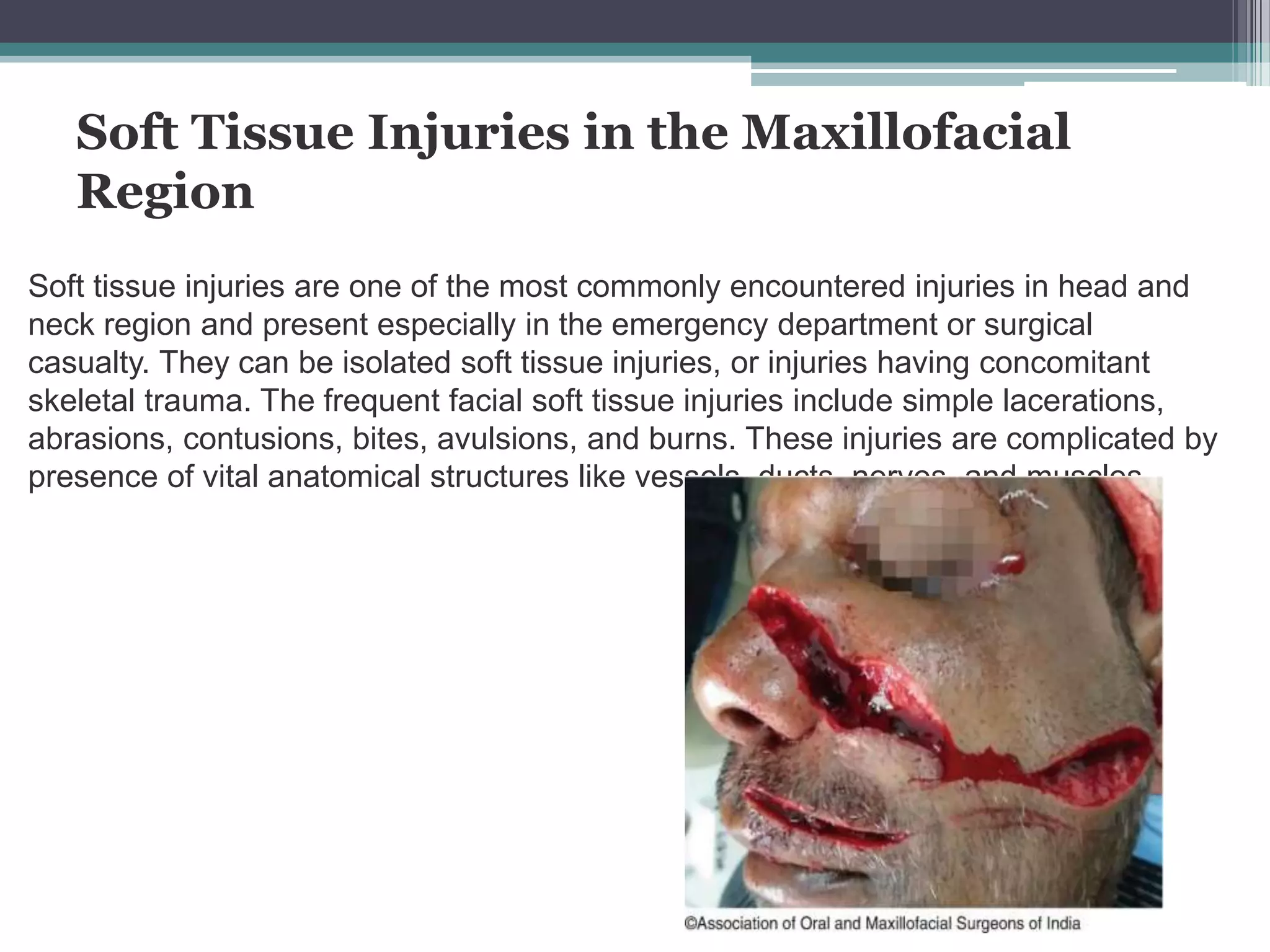
The document provides an extensive overview of maxillofacial traumatology, covering soft tissue injuries, facial fractures, and trauma to teeth and alveolar processes. It discusses various types of injuries, their causes, classifications, treatment protocols, and the importance of immediate first aid. Emphasis is placed on the complexity of maxillofacial trauma and the necessity for specialized surgical treatment to prevent complications.