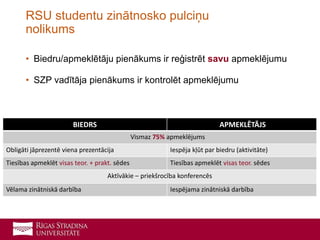
• Biedru/apmeklētāju pienākumsir reģistrēt savu apmeklējumu
• SZP vadītāja pienākums ir kontrolēt apmeklējumu
RSU studentu zinātnosko pulciņu
nolikums
BIEDRS APMEKLĒTĀJS
Vismaz 75% apmeklējums
Obligāti jāprezentē viena prezentācija Iespēja kļūt par biedru (aktivitāte)
Tiesības apmeklēt visas teor. + prakt. sēdes Tiesības apmeklēt visas teor. sēdes
Aktīvākie – priekšrocība konferencēs
Vēlama zinātniskā darbība Iespējama zinātniskā darbība
8.
• Padziļinātas zināšanasT&O nozarē
• Praktiskas iemaņas dažādās manipulācijās
• Starpkursu kontakti, domubiedri
• Iespēja izstrādāt pētniecisko darbu
• Papildus punkti regulārajai RSU stipendijai
• Akadēmiskā gada beigās – sertifikāts (punkti rezidentūrai):
• Biedriem 1.0 pts
• Apmeklētājiem 0.5 pts
Ieguvumi
• Nikola Krūmiņa
•Anna Tarasova
• Gundega Akuratere
• Uldis Spulle
• Gustavs Rindžs
• Līga Gulbe
• Uģis Šolmanis
• Anete Bērziņa
• Anna Terentjeva
• Kaspars Deičmanis
• Liene Zvaigzne
• Baiba Dace Ozoliņa
11.
• 15 minūšuprezentācija + 10-15 minūšu diskusijas daļa
• Jāiekļauj mūsdienīgu pētījumu dati
• Jāiekļauj diskusiju veicinošie elementi (piem., Case report)
• RSU prezentācijas forma (https://www.rsu.lv/par-rsu/vizuala-identitate-un-
suveniri)
• Vizuāli pārskatāms noformējums
• Visām prezentācijām jābūt iepriekš saskaņotām ar SZP vadītāju (5-10
dienas pirms sēdes jānosūta uz epastu darjaivanova4@gmail.com)
• Prezentācijas tiek grupētas atbilstoši sēdes tematikai
• Prezentācija RSU debatēs ir pielīdzināma prezentācijai pulciņa sēdē
Vispārējās prezentācijas prasības