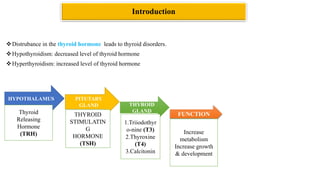
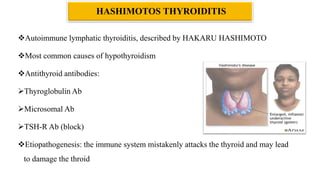
The document provides an overview of thyroid hormones, their synthesis, regulation, and associated disorders such as hyperthyroidism and hypothyroidism. It discusses the physiological roles of thyroid hormones in metabolism, growth, and development, and details various thyroid disorders, their symptoms, and management options. Additionally, it highlights the significance of conditions like Graves' disease and Hashimoto's thyroiditis in impacting thyroid function.