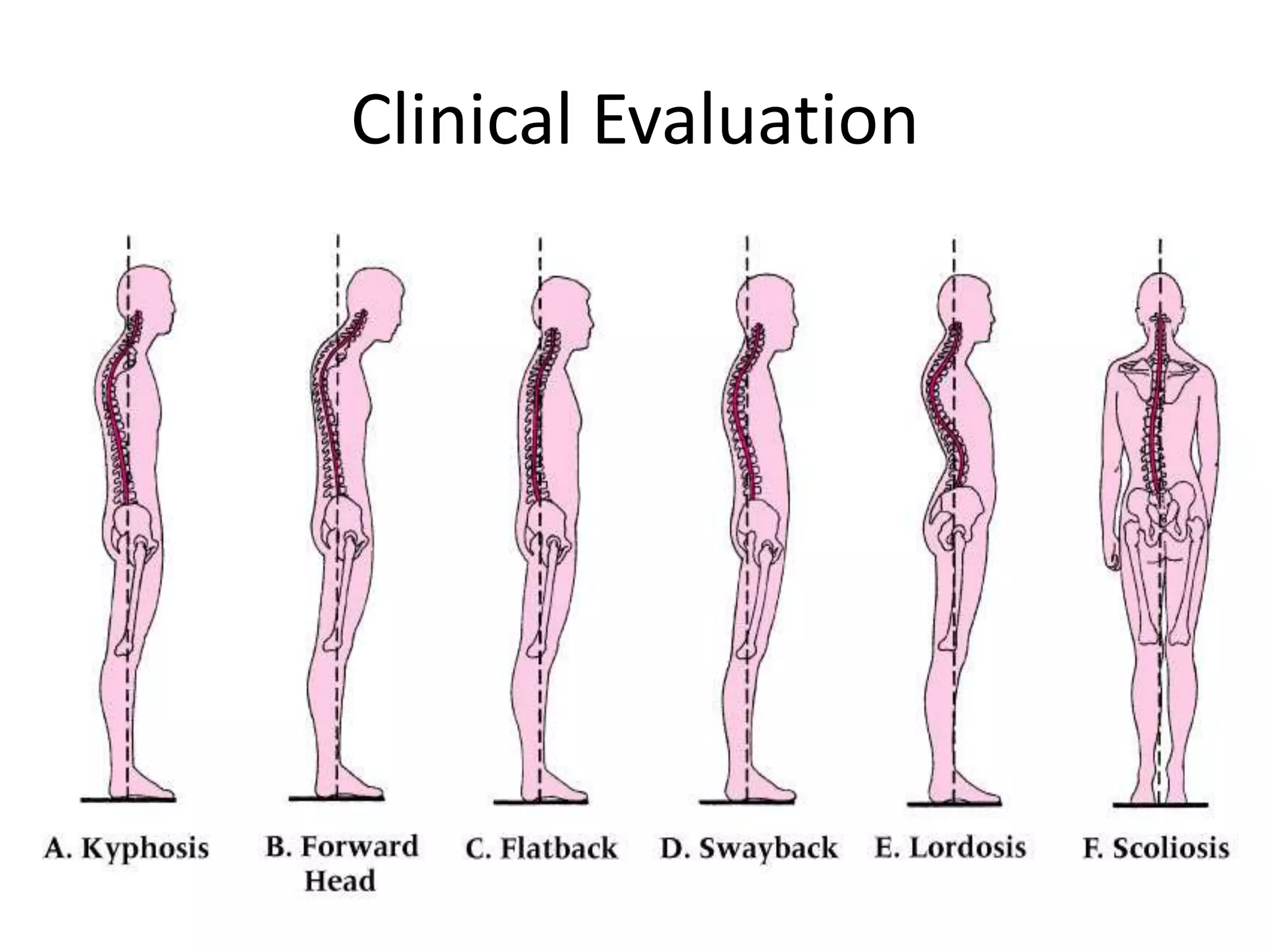
This document provides information on evaluating the thoracic and lumbar spine through clinical examination. It discusses taking a patient history including pain location and characteristics, bowel/bladder issues, and prior injuries. The physical exam involves inspecting posture, curvature, skin, breathing and palpating bony landmarks. Specific conditions like scoliosis, kyphosis and spondylolisthesis are described in terms of causes, signs, grading severity and associated symptoms.