The Mayo Clinic, known for treating international leaders,
recently saw the president of a central Africa country in its halls.
Teodoro Obiang Nguema Mbasogo, the president of the Republic
of Equatorial Guinea, was in Rochester, New York, for a checkup,
clinic officials confirmed. Security officers and limousines—not
an uncommon sight in Rochester—signaled his visit.
Nguema Mbasogo assumed the leadership of his country
with a coup that overthrew his uncle. His country recently
began working with the U.S. Agency for International Devel-
opment, under the leadership of a dean of the University of
Minnesota’s Hubert H. Humphrey Institute of Public Affairs,
to improve Equatorial Guinea’s social services. Dean J. Brian
Atwood of the institute is overseeing this effort. He went to
Equatorial Guinea in June, and a second meeting is scheduled
for this month.
The Mayo Clinic has a long international history, providing
care to international patients since its inception. Despite its his-
tory and reputation, however, the marketing staff continues to
monitor the international market to gauge the level of awareness,
reputation, and attractiveness of the Mayo Clinic around the world.
This institution has used word-of-mouth marketing to maintain its
global reputation.
Marketing, as most formally defined, historically was not a
critical factor in delivering patients to Mayo Clinic. Indeed, the
marketing department at Mayo Clinic has existed for only the past
20 years, and patients have been coming for care for more than a
century. The Clinic believes that the marketing department pro-
vides valuable information to physicians and their support staff—
information that helps them deliver better care, highlights their
patients’ wants and needs, and educates them as to what’s going
on in the marketplace.
In reality, however, it’s the providers themselves—the doctors,
nurses, receptionists, and all the rest of the allied health staff—
who bring in business by creating positive experiences for patients.
Patients who leave Mayo Clinic highly satisfied with their care
will return to their communities in the United States and elsewhere
and say good things to their family and friends. And these family
members and friends in turn travel to Mayo Clinic when they need
tertiary or quaternary medical care. Although the marketing divi-
sion strives to provide excellent internal support, it is the doctors
and other care providers who have created and maintained a brand
of healthcare excellence.
Despite the hype surrounding what has been presented as
the highly lucrative international marketplace, “international”
is not something new at Mayo Clinic. Experience and research
indicates that “international” is a part of who the Clinic is, as
well as how the market defines it. Nearly 100 years ago, the
founders, a family of physicians named “Mayo,” created an
international legacy by traveling ...
The Mayo Clinic, known for treating international leaders, .docx
1. The Mayo Clinic, known for treating international leaders,
recently saw the president of a central Africa country in its
halls.
Teodoro Obiang Nguema Mbasogo, the president of the
Republic
of Equatorial Guinea, was in Rochester, New York, for a
checkup,
clinic officials confirmed. Security officers and limousines—not
an uncommon sight in Rochester—signaled his visit.
Nguema Mbasogo assumed the leadership of his country
with a coup that overthrew his uncle. His country recently
began working with the U.S. Agency for International Devel-
opment, under the leadership of a dean of the University of
Minnesota’s Hubert H. Humphrey Institute of Public Affairs,
to improve Equatorial Guinea’s social services. Dean J. Brian
Atwood of the institute is overseeing this effort. He went to
Equatorial Guinea in June, and a second meeting is scheduled
for this month.
2. The Mayo Clinic has a long international history, providing
care to international patients since its inception. Despite its his-
tory and reputation, however, the marketing staff continues to
monitor the international market to gauge the level of
awareness,
reputation, and attractiveness of the Mayo Clinic around the
world.
This institution has used word-of-mouth marketing to maintain
its
global reputation.
Marketing, as most formally defined, historically was not a
critical factor in delivering patients to Mayo Clinic. Indeed, the
marketing department at Mayo Clinic has existed for only the
past
20 years, and patients have been coming for care for more than
a
century. The Clinic believes that the marketing department pro-
vides valuable information to physicians and their support
staff—
information that helps them deliver better care, highlights their
patients’ wants and needs, and educates them as to what’s going
3. on in the marketplace.
In reality, however, it’s the providers themselves—the doctors,
nurses, receptionists, and all the rest of the allied health staff—
who bring in business by creating positive experiences for
patients.
Patients who leave Mayo Clinic highly satisfied with their care
will return to their communities in the United States and
elsewhere
and say good things to their family and friends. And these
family
members and friends in turn travel to Mayo Clinic when they
need
tertiary or quaternary medical care. Although the marketing
divi-
sion strives to provide excellent internal support, it is the
doctors
and other care providers who have created and maintained a
brand
of healthcare excellence.
Despite the hype surrounding what has been presented as
the highly lucrative international marketplace, “international”
4. is not something new at Mayo Clinic. Experience and research
indicates that “international” is a part of who the Clinic is, as
well as how the market defines it. Nearly 100 years ago, the
founders, a family of physicians named “Mayo,” created an
international legacy by traveling around the world to compare
notes and surgical approaches with physicians across the globe.
In some cases, they even returned with international patients
who were in need of additional expertise. As in so many other
areas of medical practice, the current Mayo Clinic continues in
these traditions.
In recent years, however, it has begun to study the international
patient population in particular and the international
marketplace
in general. These studies fall into a few categories and grow in
number in proportion to the organization’s understanding (or
per-
haps greater understanding of how much it does not know) of
the
international marketplace.
First, the Mayo Clinic tracks international patient trends rather
5. carefully, which seems like an obvious place to start. But as in
most data tracking, the value of the concept is significantly
more
straightforward than the logistics of acquiring consistently
reliable
data. Internal data systems must be coordinated—a significant
undertaking for any institution, and particularly hard when deal-
ing with a large and complicated infrastructure. To give a
simple
example, data fields must be made uniform—not just on one
data
system, but on all of them. Rather than a free-text field, for
exam-
ple, that allows a registrant to enter Venzuela, or Venosuela, or
Vensuala, or maybe even Venezuela, the Mayo Clinic pushes for
a
predefined field that provides standardized information.
The Clinic monitors international data by the quarter, carefully
watching trends over time by country or region, tracking
signifi-
cant changes in volume, hospitalization rates, and percentage of
6. new patients out of any given market. For example, it knows it
has between 9,000 and 10,000 patients, depending on the year,
from more than 160 different countries annually. Some are
third-
generation patients—maybe their grandfather was cured there in
the 1930s—and others are brand new. Some are neighbors from
Ontario or Monterrey; others come all the way from Indonesia.
Some markets are significantly less predictable than others, and
some countries deliver more “new” patients than others. The
Mayo
Clinic probes further to figure out why.
Second, it conducts research with internal salespeople—the
physicians and their support staff who deliver care to
international
patients. Through carefully moderated focus groups, the Clinic
identifies the things that are going smoothly, as well as the
barri-
ers to providing excellent care. And where appropriate, it makes
recommendations for change.
Third, just as with U.S.-based patients, the healthcare insti-
7. tute conducts both quantitative and qualitative research in the
international marketplace, including research with patients,
international physicians, and international healthcare con-
sumers, designed to help it understand why people choose to
leave their own communities for healthcare, why some of them
come to Mayo Clinic, and why others do not. It works hard to
understand how healthcare decisions are made so it can better
assist decision makers, physicians, and their staff in providing
care. The Clinic positions itself to offer counsel on where to
best expend valuable institutional resources, both human and
financial.
GLOBAL MARKET RESEARCH
The marketing department conducts periodic and ongoing
patient
satisfaction studies with international patients, measuring their
assessment of various aspects of the care provided. To date, the
International Marketing Research
at the Mayo Clinic
CASE 3-1
8. Cases 3 Assessing Global Market Opportunities
Mayo Clinic has surveyed nearly 1,500 patients in 20 countries,
in
four different languages. As any market researcher knows,
sound
patient satisfaction research requires great attention to detail to
ensure reliable data. Not surprisingly, international data
collection
offers significant additional challenges. For example, according
to
the Mayo Clinic:
The quality of our own data. The name and address fields
designed for clean U.S. addresses often are not sufficient to
hold reliable international detail. If we want to do it right,
we must manually “clean” thousands of patient records be-
fore fielding our studies.
Varying quality of international postal and telecommuni-
cations infrastructure. This variance can create significant
problems for either phone or mail surveys; consequently,
9. international studies take a lot more time than U.S.-based
studies and require much more patience.
Cultural dynamics. In some countries, individuals may be
suspicious of an international call; in others, they may spend
a lot of time outside of their homes. In still others, a nonfam-
ily “gatekeeper” must be diplomatically convinced to transfer
the call to the targeted respondents. These cultural dynamics
pose further delays and require special sensitivities.
High standards for quality. Our own standards for quality
compel us to maintain high quality language- and culture-
specific fielding of our various research projects. These
studies, whether managed internally or through an external
vendor, require more oversight than we are accustomed to
with U.S.-based research.
Despite these challenges, however, this international research
has taught the Mayo Clinic a lot. International patient
satisfaction
studies demonstrate that the key driver of patients’ satisfaction
seems to hold across borders. This is excellent care—manifested
10. by listening, explaining, and thoroughness on the part of Mayo
Clinic physicians. Other factors in the healthcare experience are
important—for example, quality of language interpretation and
waiting times—but they do not consistently correlate with
overall
satisfaction.
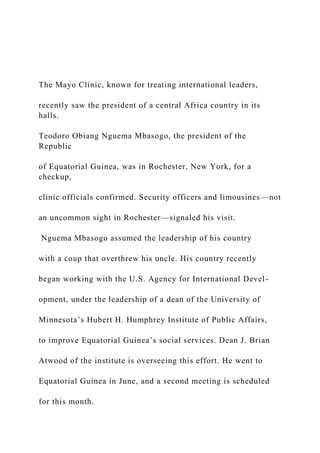
The power of word of mouth is also confirmed in the inter-
national marketplace. Most international patients indicate that
friends or relatives provided their most important influence in
choosing Mayo Clinic. This finding reinforces the most
powerful
marketing “tool”—satisfied patients who say good things about
Mayo Clinic and influence others’ healthcare decisions. Exhibit
1
indicates the factors influencing choice of Mayo Clinic by
patients
from Latin America and the Middle East.
Formal focus groups with international patients and nonpa-
tients in six cities around the world attempted to learn more
about
11. how those populations make healthcare decisions, and whether
the
process is the same or different from U.S. healthcare
consumers.
As it turns out, for most aspects of decision making, the process
is
very similar to that of U.S. consumers. However, for a few
others,
the process is quite different.
The areas with the most differences across borders relate to the
role of health insurance. Three co-sponsored international
research
projects have provided some good lessons and demonstrated that
international healthcare insurance is as different from that in
the
United States as it is across countries and regions. Furthermore,
many assumptions taken for granted in the U.S. market—for
exam-
ple, name recognition—simply do not hold in certain
international
markets. Exhibit 2 is a graph of responses from a satisfaction
study
of patients from Latin America and the Middle East, showing
12. the
different history of Mayo Clinic brand awareness in those
regions
Mayo Clinic awareness among patients was much more recent
in the Middle East than in Latin America. Other studies,
however,
showed that awareness among nonpatients—even those who
have
purchased health insurance policies that offer them Mayo Clinic
care as a benefit—is not as strong.
The international healthcare insurance market is expanding
rapidly, and many providers view this expansion as a significant
opportunity to glean additional patients from outside the United
States. Commercial and noncommercial contracts comprise a
significant body of business in U.S. healthcare. If this business
could be expanded to provide patients from markets outside the
United States, all the better. However, healthcare systems vary
significantly from country to country, and the knowledge and
use
of health insurance vary even more. To study these
differences in
13. Exhibit 1
Which Was Most
Important in Your Decision
to Choose Mayo Clinic?
International Patient Satisfaction
N 5 331 Middle Eastern patients; 755 Latin American patients.
0% 10% 20% 30% 40% 50% 60% 70%
Friend or
relative
Media (TV, radio,
newspaper)
Internet
Government
Doctor
at home
Other
Latin America
Middle East
Part 6 Supplementary Material
detail, the Mayo Clinic cosponsored two quantitative studies of
14. healthcare insurance policyholders—in particular, holders of
pol-
icies that offer some degree of coverage for care at Mayo
Clinic.
The first study consisted of face-to-face interviews with
400 policyholders in a particular country and delivered a great
deal
of information regarding policyholders’ preferences, healthcare
behavior, and demographics. In this country, as throughout most
of
the world, the public healthcare system exists as a universal
“safety
net” for all citizens. Even in markets where the private
insurance
market has expanded, the public system continues to offer care
for
all citizens. Therefore, if a private insurance policy does not
offer
adequate coverage, especially for high-cost procedures, the
public
system is used to reduce the consumer’s financial burden.
The private policy might cover, for example, access to primary
15. and secondary care at private rather than public clinics as well
as the price of a private room, or the option of receiving care at
a more upscale facility. But for high-cost, life-threatening pro-
cedures, the co-pay or deductible for having these procedures
conducted exclusively in the private sector remains significant.
The end result, of course, is that the lower cost procedures are
transferred to the private system, while the higher cost
procedures
remain in the public safety net. The implication for U.S. tertiary
providers is that, while private insurance might reduce some of
the
financial risk for traveling out of country for care, in many
cases
the risk is not completely eliminated. Therefore, the policies
might
not deliver the volume of patients initially anticipated.
Other factors, such as a lack of brand awareness and limited
perceived need for U.S. medical care, may be impediments to
attracting patients in the international healthcare insurance mar-
ket. In the first study, when the Clinic probed for brand
awareness
16. among those 400 consumers who had purchased a health insur-
ance policy touting Mayo Clinic coverage as a benefit, no
unaided
recall of that coverage emerged as a benefit of the policy. (See
Exhibit 3.) In an aided list, Mayo Clinic coverage was ranked as
the least important benefit of the policy, on a par with eyeglass
coverage at the bottom of the list.
Furthermore, when asked to name a leading medical center in
the United States, most policyholders (72 percent) did not know
a
single one. Twenty-five percent (25 percent) named Mayo
Clinic,
and the other 2 percent named other U.S. medical centers. It
was
no real surprise that citizens in the studied country were not
famil-
iar with Mayo Clinic. However, the Clinic was surprised that
policyholders who had purchased an insurance product that very
publicly advertised the Mayo Clinic benefit were unable to
name
Mayo Clinic as a leading U.S. medical center.
17. As it turned out, many of these policyholders had no intention
of leaving their home country for medical care. They were
buying
insurance to facilitate care in the more desirable private system.
Furthermore, most felt that the healthcare in their own country
was very good and that there would be little if any reason to
ever
leave home to obtain care elsewhere. This phenomenon emerges
repeatedly in research with U.S. patients. Most believe in the
abili-
ties of their own doctor and feel very confident about medical
care
in their own community. Even though “quality” may be
regionally
or culturally defined, almost everyone considers his or her
doctor
to be a good one.
A second cosponsored study consisted of 353 telephone inter-
views with individuals who had purchased a healthcare
insurance
policy specifically for international coverage. Once again,
confi-
18. dence in local care was very high—in fact, significantly higher
than in the country of the first study. Nonetheless, this group of
individuals had purchased a product that offered them coverage
for medical care outside their home country, should they decide
it
was necessary or appropriate. In this study, aided brand
recogni-
tion among policyholders was higher than in the first; when
asked directly whether they had heard of Mayo Clinic, 75
percent
responded affirmatively. But when asked unaided to name the
best medical centers in the United States, the vast majority
(nearly
70 percent) of policyholders indicated they did not know. And
while the majority had heard of Mayo Clinic, fewer than 10
percent
were aware of any benefit of their health insurance policy that
related to Mayo Clinic.
Exhibit 2
How Long Ago Did You First Hear of Mayo Clinic?
International Patient Satisfaction
19. N 5 331 Middle Eastern patients; 755 Latin American patients.
0% 10% 20% 30% 40% 50% 60% 70%
For as long as
I can remember
Within past 2–5 years
Within past 1–2 years
Within past year
Latin America
Middle East
Cases 3 Assessing Global Market Opportunities
Both of these studies offered substantially more information
about the nature of international insurance agreements, policy-
holders’ wants and needs, and their disposition toward traveling
out of country for medical care. But they also showed that the
knowledge of the Mayo brand is limited outside the United
States
and that a high number of policyholders does not necessarily
translate into a high number of patients. This research has
20. taught
the Clinic to be more selective, to be cautious in expending
signifi-
cant resources to pursue insurance arrangements, and to conduct
further research to expand understanding.
THE FUTURE
“International” will continue to be part of who the Mayo Clinic
is. Its doctors, hailing from all corners of the globe, will
continue
to collaborate with their colleagues around the world. Mayo
Clinic researchers will conduct clinical trials in collaboration
with researchers on many continents. Students and residents
will continue to offer rich diversity, as Mayo international
alumni now number 1,500, representing 67 countries. But most
important, Mayo Clinic will strive to provide the best medical
care possible to those patients around the world who need it
the most.
To support that mission, members of the “marketing” depart-
ment will continue to support the medical staff by studying
21. Exhibit 3
Recall of Plan Benefits (unaided)
N 5 400 individuals who had purchased a health insurance
policy advertising Mayo Clinic coverage as a benefit.
0% 10% 20% 30% 40% 50% 60% 70%
Hospitalization
Consult reimbursement
Exams/X-rays/lab tests
General medicine
Ambulatory coverage
High reimbursement %
Serious illness
Can choose clinic
patients’ wants, needs, preferences, and behavior patterns and
learning all that they can about the ever-changing, rich, and
diverse
worldwide healthcare market. In the end, outstanding medical
care and sensitive service to patients and families will be the
most
productive marketing strategy, because it creates positive word
22. of mouth about something very important—healthcare. As the
stories of satisfied patients churn—sometimes for decades—in
the
minds of their friends and family, Mayo Clinic remains an
option
if they ever need the care it offers.
QUESTION
Assume you are the new marketing vice president at the Mayo
Clinic. The CEO and the board have decided to expand their
international sales revenues by 100 percent over the next five
years.
Write a memo to your staff outlining the marketing research
that
will be needed to support such a strategy. Be specific about
sources
of secondary data and the best places and media for gathering
primary data. Also, be specific about the best methods to use.
Sources: Misty Hathaway and Kent Seltman, “International
Marketing Research
at the Mayo Clinic,” Marketing Health Services, Winter 2001,
21(4), pp. 18–23;
Jeff Kiger, “African President Gets Checkup at Mayo Clinic,”
23. Post-Bulletin,
September 21, 2007; “Mayo Clinic Builds Center for
International Patients,”
Post-Bulletin, February 3, 2009.
Criteria Achievement Level
Unacceptable(0%)
Needs
Improvement
(33%)
Good
(67%)
Excellent
(100%)
SWOT Analysis
(10% Weighting)
0 percent
The SWOT analysis is
either very poorly
done (>5 things
wrong with it) or
missing, and/or the
explanation is
missing.
24. 3 percent
A SWOT analysis is
presented and
explained, but there
are 3-4 things wrong
with the analysis
and/or the
explanation is very
unclear.
7 percent
A SWOT analysis is
presented and
explained, but there
are 1-2 things wrong
with the analysis—
e.g., at least one major
item is missing, or an
item is inappropriately
categorized, or an
opportunity is written
as a tactic.
Alternatively, the
explanation of the
SWOT may be
unclear.
10 percent
A thorough SWOT
analysis is presented
and explained. There
are no major
strengths, weaknesses,
opportunities, or
threats missing. In
addition, items under
25. each category are
appropriately
categorized and
written
Identification of
Problems/Issues
(20% Weighting)
0 percent
The problem
identification is
missing or not based
on SWOT analysis at
all. In addition, there
is no attention given
to relationships
among and
prioritization of
problems. Shows lack
of judgment.
7 percent
Problem and issue
identification is
unclear in some
aspects and is not
wholly based on
SWOT analysis.
Prioritization is
confused.
Relationships and
the key underlying
problem/issue are
either misidentified
or missing.
26. 13 percent
Problem and issue
identification is clear,
based on the SWOT
analysis, and
prioritizations have
been made. Most, but
not all, judgments
about priorities are
appropriate.
Relationships and the
key underlying
problem/issue are
identified.
20 percent
Clearly identifies
problems/issues,
based on the SWOT
analysis. The
problems/issues are
prioritized,
differentiating those
that are important
from those that are
routine. Relationships
among the problems
are identified, with the
underlying, primary
or key problem/issue
clearly designated.
Identification
and Analysis of
27. 0 percent
Either the list of
alternative actions is
missing or the list is
very incomplete or
there is no linkage of
the alternative actions
to the SWOT or to the
problems/issues. None
of the alternatives
identifies a broad
strategic direction.
Shows lack of
thorough
consideration.
10 percent
The list of
alternative actions is
incomplete or
unclear in some
aspects, and includes
alternatives that are
not based on the
SWOT and/or are
not reasonably
linked to the
problems and issues.
More than one
alternative is too
narrow and does not
20 percent
Identifies alternative
actions that can be
taken to address
28. problems/issues.
Most, but not all,
alternative actions are
linked to the SWOT
and problems/issues.
Alternative actions is
very narrow (tactical)
and does not identify
a broad strategic
direction. Analysis of
alternative actions is
30 percent
Clearly identifies
several alternative
actions that can be
taken to address
problems/issues. The
list of alternatives is
complete and linkage
to the SWOT and
problems/issues is
clear, providing clear
reasoning for
inclusion as an
alternative action.
Analysis of alternative
Alternative
Actions
(30% Weighting)
Analysis is trivial or
29. missing, lacking any
depth. No
assumptions are stated
(& are needed).
Likely
benefits/disadvantages
are not provided at all
or are unsupported by
the analysis.
identify a broad
strategic direction.
Some analysis is
included, but it is not
very detailed. Many
statements are not
supported by
analysis/calculations.
Most of the stated
assumptions are not
justified. Several
benefits/
disadvantages are
missing and/or not
clearly identified or
unsupported by the
analysis.
detailed, but some
statements are
unsupported by
analysis/ calculations.
Assumptions are
stated, but some are
not justified. Most,
but not all,
30. benefits/disadvantages
are clearly identified
and supported by the
analysis.
actions is detailed.
Any necessary
assumptions are stated
and justified. The
analysis appropriately
incorporates strategic
marketing
management concepts
and financial analysis.
The likely
benefits/disadvantages
of each action are
clearly identified and
supported by the
analysis.
Recommendation
(30% Weighting)
0 percent
A solution is
recommended, but it
is not derived from
the alternative
analysis at all; or the
recommended
solution is clearly not
viable, given the
SWOT analysis; or
the recommended
solution does not
31. address the
problems/issues; or
there is no
recommended
solution.
10 percent
A solution is
recommended, but
logical derivation
from alternative
analysis is unclear,
and there is clearly a
better optimal
solution, given the
SWOT analysis. The
recommendation is
based on more than
one alternative
action. No
identification of
assumptions,
caveats, or
considerations that
might affect the
recommendation is
provided.
20 percent
An action plan is
given, which is
mostly, but not
completely, logically
derived from
alternative analysis.
There may be a better
32. solution to the
problems/issues than
the one
recommended, given
the SWOT analysis.
Most, but not all,
assumptions, caveats,
and ongoing
considerations are
provided.
30 percent
A clear action plan is
given, logically
derived from
alternative analysis,
that provides optimal
solution for identified
problems/issues and
that further makes
sense, given the
SWOT analysis; the
recommendation is
based on only one of
the alternative actions.
Assumptions, caveats,
ongoing
considerations
concerning
recommendation are
provided.
Organization
(5% Weighting)
0 percent
33. The case analysis is
disorganized to the
extent that it prevents
understanding of
content. There are no
headings. There is no
introduction. There
are no page numbers.
2 percent
The organization is
unclear; headings are
missing. The
introduction is not
succinct. Page
numbers may be
missing.
3 percent
The organization is
generally good. There
is a brief introduction
and section headings;
there are page
numbers. But some
sections seem out of
place or mislabeled,
diminishing the ease
with which the case
reads and is
understood.
5 percent
Written work is well
organized and easy to
understand. There is a
34. brief introduction.
Sections of case
analysis are marked
with appropriate
headings. There are
page numbers.
0 percent 2 percent 3 percent 5 percent
Integration of
Business Writing
(5% Weighting)
Writing is
unacceptable.
The writing fails to
comply with all six
criteria for business
writing as discussed
in the on ANGEL.
The writing complies
with some of the
criteria for business
writing as discussed
in the handout on
ANGEL.
The writing complies
with all six criteria for
business writing as
discussed in the
handout on ANGEL.