Meghan Hoyer: "Will the Silver Tsunami Send Medicare into the Red?" 12.17.15reportingonhealth
Meghan Hoyer's slides from the Center for Health Journalism webinar "Will the Silver Tsunami Send Medicare into the Red?" 12.17.15
http://www.centerforhealthjournalism.org/content/will-silver-tsunami-send-medicare-red
Dr. Mollyann Brodie: "What Soaring Drug Prices Mean for Patients," 9.3.15reportingonhealth
Dr. Mollyann Brodie's presentation from "What Soaring Drug Prices Mean for Patients," 9.3.15
http://www.reportingonhealth.org/content/what-soaring-drug-prices-mean-patients
Eugene Steuerle: "Will the Silver Tsunami Send Medicare into the Red?," 12.17.15reportingonhealth
Eugene Steuerle's slides from the Center for Health Journalism webinar "Will the Silver Tsunami Send Medicare into the Red?" 12.17.15
http://www.centerforhealthjournalism.org/content/will-silver-tsunami-send-medicare-red
Meghan Hoyer: "Will the Silver Tsunami Send Medicare into the Red?" 12.17.15reportingonhealth
Meghan Hoyer's slides from the Center for Health Journalism webinar "Will the Silver Tsunami Send Medicare into the Red?" 12.17.15
http://www.centerforhealthjournalism.org/content/will-silver-tsunami-send-medicare-red
Dr. Mollyann Brodie: "What Soaring Drug Prices Mean for Patients," 9.3.15reportingonhealth
Dr. Mollyann Brodie's presentation from "What Soaring Drug Prices Mean for Patients," 9.3.15
http://www.reportingonhealth.org/content/what-soaring-drug-prices-mean-patients
Eugene Steuerle: "Will the Silver Tsunami Send Medicare into the Red?," 12.17.15reportingonhealth
Eugene Steuerle's slides from the Center for Health Journalism webinar "Will the Silver Tsunami Send Medicare into the Red?" 12.17.15
http://www.centerforhealthjournalism.org/content/will-silver-tsunami-send-medicare-red
Larry Levitt: "Out of Pocket: Surprise Costs After Health Reform," 10.29.15reportingonhealth
Larry Levitt's presentation from "Out of Pocket: Surprise Costs After Health Reform," 10.29.15
http://www.reportingonhealth.org/content/out-pocket-surprise-costs-after-health-reform
Zack Cooper: "Inside the ‘Black Box’ of Health Care Spending Data?" 2.18.16reportingonhealth
Zack Cooper's slides from the Center for Health Journalism webinar "Inside the ‘Black Box’ of Health Care Spending Data," 2.18.16
http://www.centerforhealthjournalism.org/content/inside-black-box-health-care-spending-data
Economic Impact on Minnesota's Health Care Delivery Systemsoder145
Presentation by Lynn Blewett to the Minnesota State Legislature at a joint meeting of the health care and human services finance and policy committees in Saint Paul, MN, February 10 2009.
Larry Levitt: "Out of Pocket: Surprise Costs After Health Reform," 10.29.15reportingonhealth
Larry Levitt's presentation from "Out of Pocket: Surprise Costs After Health Reform," 10.29.15
http://www.reportingonhealth.org/content/out-pocket-surprise-costs-after-health-reform
Zack Cooper: "Inside the ‘Black Box’ of Health Care Spending Data?" 2.18.16reportingonhealth
Zack Cooper's slides from the Center for Health Journalism webinar "Inside the ‘Black Box’ of Health Care Spending Data," 2.18.16
http://www.centerforhealthjournalism.org/content/inside-black-box-health-care-spending-data
Economic Impact on Minnesota's Health Care Delivery Systemsoder145
Presentation by Lynn Blewett to the Minnesota State Legislature at a joint meeting of the health care and human services finance and policy committees in Saint Paul, MN, February 10 2009.
Harvard's Robert Greenwald on Texas MedicaidOneVoiceTexas
Robert Greenwald, JD, Clinical Professor of Law and Director of Center for Health Law and Policy Innovation at Harvard Law School, presented an in-depth analysis forum of the federal health reform Affordable Care Act and associated transformation of the Texas Medicaid system. On January 24 in Austin, he spoke to sever audiences on the challenges and opportunities specific to Texas including why the Affordable Care Act’s Medicaid expansion is so important to the provision of cost- effective, high quality care and treatment to low income uninsured Texans.
Professor Greenwald has over 20 years of experience in the fields of health law and policy. His Center is recognized as a national leader in Affordable Care Act implementation and in efforts to improve healthcare access and health outcomes for the uninsured and underinsured.
One Voice Texas and the Harris County Healthcare Alliance sponsored the event.
PERSPECTIVEn engl j med 368;6 nejm.org february 7, 2013496.docxmattjtoni51554
PERSPECTIVE
n engl j med 368;6 nejm.org february 7, 2013496
for aging. Highlighting the field’s
orphan status, a decade-long ini-
tiative by the Substance Abuse and
Mental Health Services Adminis-
tration implementing evidence-
based geriatric mental health
and substance-abuse programs
throughout the country was re-
cently eliminated, just as the
wave of Baby Boomers turning
65 began to crest.1 On the re-
search front, National Institutes
of Health policy has inexplicably
allowed the systematic exclusion
of study participants over 65
years of age in federally funded
research involving adults (but re-
quires detailed justification for
research that excludes women,
minority groups, and children).
This policy forces clinicians to
extrapolate from findings on the
safety and effectiveness of treat-
ments that have been tested only
in younger adults, and it perpetu-
ates what has been called the “ev-
idence-free” practice of geriatrics.
We believe that steps should be
taken to mandate the inclusion of
older adults in federally funded
research unless there is scientific
justification for excluding them,
and we agree with the IOM that
immediate steps are needed to re-
store the national program sup-
porting the implementation of
geriatric community mental health
and substance-use programs.
Emerging Medicare accountable
care organizations should inte-
grate geriatric mental health and
substance-use expertise as com-
ponents of health coaching and
chronic disease management for
patients with complex, high-cost
health conditions. The potential
for prevention must also be
tapped, in part through the adop-
tion of evidence-based psycholog-
ical interventions that reduce the
incidence of depression among
patients with health conditions
associated with greater risk, such
as stroke and macular degenera-
tion. Finally, the fragmentation and
neglect of services and research
may be addressed by creating a
dedicated federal office responsi-
ble for overseeing funding and
coordination across the different
agencies responsible for aging,
mental health, and substance-use
disorders.
Although these reforms are
necessary first steps, they will be
insufficient without dramatic
changes in what we do and how
we do it. If we recognize that
mental health care is a core com-
ponent of general health care for
aging Americans and transform
the health care workforce ac-
cordingly, there may be hope that
we can weather the approaching
“silver tsunami.”
Disclosure forms provided by the authors
are available with the full text of this article
at NEJM.org.
From the Departments of Psychiatry and of
Community and Family Medicine, Geisel
School of Medicine at Dartmouth, Ha-
nover, NH (S.J.B.); and the Dartmouth In-
stitute for Health Policy and Clinical Prac-
tice, Lebanon, NH (S.J.B., J.A.N.).
This article was published on January 23,
2013, and updated on February 7, 2013, at
NEJM.org.
1. Institute of Medicine. Th.
You should respond to at least two of your peers by extending- refutin.docxjosee57
You should respond to at least two of your peers by extending, refuting/correcting, or adding additional nuance to their posts.
Post #1
Jenna Horgan
NUR 420
Professor Roberts
January 12, 2023
Who are the clients in Community Health nursing?
Individuals, families, and groups who live in a specific geographic area and may be at risk for health problems or in need of health services are considered clients in community health nursing. People of all ages, from infants to the elderly, as well as those with physical, mental, or social challenges, may be included. The purpose of community health nursing is to promote the health and well-being of the entire community by addressing the health needs of its individual members (Rector & Stanley, 2021). Community health nurses work with clients to identify and address health risks, provide health and wellness education, and connect clients to suitable health services.
What government resources might they be eligible for?
Individuals and families may be eligible for a variety of government resources depending on their circumstances. Some of these resources are intended specifically for people with low incomes or who are experiencing financial hardship, while others are open to anyone who meets certain criteria. Among the resources available to them are (ISPOR, n.d):
1. Medicaid: It is a federal-state partnership program that provides health insurance to low-income individuals and families. Individuals must meet income and asset limits, as well as other requirements, to be eligible.
2. Children's Health Insurance Program (CHIP): It is a federally funded program that provides health insurance to low-income children that are not eligible for Medicaid but cannot afford private health insurance. It provides coverage for a variety of medical services, such as preventive care, doctor visits, hospital stays, and prescription medications. Eligibility is determined by income and family size.
3. Supplemental Nutrition Assistance Program (SNAP): It is also known as food stamps and it provides financial assistance to low-income individuals and families in order for them to purchase food. Income and assets, as well as other factors, determine SNAP eligibility.
4. Temporary Assistance for Needy Families (TANF): This program helps low-income families with children by providing financial assistance as well as other services such as job training and childcare. Income and assets, as well as other factors, determine TANF eligibility.
5. Low Income Home Energy Assistance Program (LIHEAP): It is program funded by the federal government that provides low-income households with financial assistance to help them pay for home energy costs such as heating and cooling. The Department of Health and Human Services (HHS) administers the program, which is intended to assist households that are struggling to pay their energy bills and may face having their service disconnected. Eligibility is determined by income and family size.
What ag.
Running head THE DETERMINATION OF ELIGIBILITY FOR MEDICAID .docxtoltonkendal
Running head: THE DETERMINATION OF ELIGIBILITY FOR MEDICAID 1
THE DETERMINATION OF ELIGIBILITY FOR MEDICAID 6
The Determination of Eligibility for Medicaid
Tiffany Williams
The Determination of Eligibility for Medicaid
Introduction
The social health care program, Medicaid is aimed at providing health care services to the needy and those with disabilities in the United States. The Act should provide the state with the way forward or criteria to be followed in selecting the people who are to benefit from the social health program. However, over time, it has not been clear to every American citizen as to which criteria should be used in determining the needy in the society. In particular, it has been challenging on selecting the eligible citizens for the program with a focus on the level of income and the level of expenditure. For instance, the issue of “spend down” periods has posed a lot of difficulties in determining the eligibility for Medicaid. A way great issue regarding the funding, expansion, and determination of eligibility for Medicaid includes the requirement by the Supreme Court in the United States for regions such as Massachusetts to contribute the six months’ excess income towards medical expenditure before the Medicaid coverage program begins in such regions. This paper seeks to explain the issue of Medicaid coverage and the eligibility of the different level of community members. It also explores the level of government affected by the issue as well as the analysis of the eligibility of Medicaid.
Economic Issue
The social health program (Medicaid) requires adequate funding in order to cover effectively a large and needy population. While it would be more beneficial to expand the program to the other categories of people in the society such as those with disabilities, there should be constant and enough supply of funds both from the government and the good wishers such as donors to help reach out every needy member of the society. Inadequate funding is an issue since there is a large percentage of people who need medical assistance and cannot afford it unless they get subsidized medical health care or fully assisted by programs such as the Medicaid (Ford, Spicer, & Institute of Medicine (U.S.), 2012).
Coupled with the low income of most of the society members, it is clear and evident enough that the majority of the people in the United States value social programs such as Medicaid. However, failure to adequately fund the program has only led to development and implementation of strict procedures and regulations in determining those who are eligible for the program. In particular, the six-month spend down period has resulted in more complex procedures, some of which are neither clear nor understandable to society members. The methodology used has never been friendly to the low-income people; the approach involving spend down for ...
Virginia AFP's lobbyist Hunter Jamerson's presentation from the 2013 SLC on the unique Medicaid reform approach being followed in the state of Virginia.
Donor Government Disbursements for Family Planning in 2017 (Slideshow)KFF
Donor government funding for family planning increased in 2017, rising from $1.20 billion in 2016 to $1.27 billion (an increase of $74 million or 6%, as measured in current terms); funding increased even after accounting for inflation and currency fluctuations.
2019 KFF Employer Health Benefits Survey ChartpackKFF
The 2019 Employer Health Benefits Survey finds annual family premiums for employer health insurance rose 5% to average $20,576 this year. On average, workers pay $6,015 toward the cost.
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
The POPPY STUDY (Preconception to post-partum cardiovascular function in prim...
The ACA and LGBT Individuals - New Options for Coverage and Care
1. The ACA and LGBT Individuals:
New Options for Coverage & Care
Jen Kates, PhD
May 20, 2014
Vice President; Director, Global Health & HIV Policy
Kaiser Family Foundation
@jenkatesdc
3. • Medicaid expansion to nearly all
low income individuals (up to
138% FPL) in states opting to
expand
• Health insurance marketplaces
in every state, with subsidies for
those who are low income
• Medicaid: Supreme Court decision
made Medicaid expansion a state
option
• Marketplaces: Plans must meet
federal standards but vary
significantly in terms of provider
networks, benefit packages, etc.
Provision Issues to Consider
• 10 Essential Health Benefits (EHB)
categories, including preventive
services, mental health/substance
use, prescription drugs
• Preventive services include HIV &
STD screening, immunizations,
other chronic disease screenings
• Preventive Services: all USPSTF “A”
and “B” rated services must be
provided at no cost in all non-
grandfathered health plans and for
Medicaid expansion population in
states that expand
Overview of Changes due to the ACA
Expanded
Access to
Coverage &
Market
Reforms
Preventive
Services/
Benefits
Standards
NOTES: USPSTF = U.S. Preventive Services Task Force; FPL = Federal Poverty Level.
SOURCES: Ranji U, Beamesderfer A, Kates J, Salganicoff A, Health and Access to Care and Coverage for Lesbian, Gay, Bisexual, and Transgender Individuals in the
U.S., Kaiser Family Foundation, January 2014; Cray A, Baker K, How the Affordable Care Act Helps the LGBT Community, Center for American Progress, May 2013.
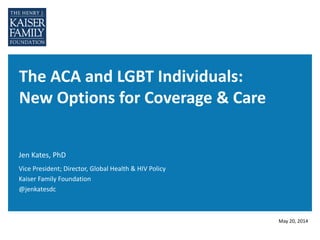
4. Figure 3
NOTES: Data are as of April 2014.
SOURCES: KFF, State health facts, http://kff.org/health-reform/state-indicator/state-activity-around-expanding-medicaid-under-the-affordable-care-
act/#notes; KFF analysis of data from CDC; personal communication with Kellan Baker, Center for American Progress, May 2014.
WY
WI*
WV
WA
VA
VT
UT
TX
TN
SD
SC
RI
PA
OR
OK
OH
ND
NC
NY
NM
NJ
NH*
NV
NE
MT
MO
MS
MN
MI*
MA
MD
ME
LA
KYKS
IA
INIL
ID
HI
GA
FL
DC
DE
CT
CO
CA
AR*AZ
AK
AL
Implementing Expansion in 2014 (27 States including DC)
Open Debate (5 States)
Not Moving Forward at this Time (19 States)
Status of State Medicaid Expansion Decisions, 2014
41% LGBT,
44% PLWHA
live in states
not expanding
5. • End to pre-existing condition
exclusions (cannot be charged
more for being LGBT, HIV+)
• Section 1557 prohibits
discrimination based on sex,
(includes Gender ID, sex
stereotypes), in any health
program receiving federal funds
• Plans offering EHB barred from
discriminating based on sexual
orientation and gender identity
(SOGI)
• Health plans outside
marketplace required to offer
married same sex spouses
coverage if offered to opposite
sex spouses (as of 2015)
• Section 1557 not currently
interpreted to include sexual
orientation
• While transgender individuals
should have access to needed
services if covered for others in
health plan, plans can still exclude
care related to gender transition
• Seven states offer SOGI insurance
protections (CA, CO, CT, DC, MD,
OR, VT).
Provision Issues to Consider
Overview of Changes due to the ACA, continued
Non-
Discrimination
Provisions
SOURCES: Ranji U, Beamesderfer A, Kates J, Salganicoff A, Health and Access to Care and Coverage for Lesbian, Gay, Bisexual, and Transgender Individuals in the
U.S., Kaiser Family Foundation, January 2014; Cray A, Baker K, How the Affordable Care Act Helps the LGBT Community, Center for American Progress, May 2013.
6. • ACA calls for routine data
collection/surveillance on
health disparities, including for
LGBT populations; also Healthy
People 2020 goal
• Sexual orientation question
added to NHIS
• CDC approved SOGI questions
for state-administered BRFSS
• SOGI metrics in Electronic
Health Records (meaningful use
standards)
Provision Issues to Consider
Overview of Changes due to the ACA, continued
Data
Collection &
Research
• Still not routine for researchers
and health data systems to
collect and report SOGI data
NOTES: NHIS = National Health Interview Survey; BRFSS = Behavioral Risk Factor Surveillance System
SOURCES: Ranji U, Beamesderfer A, Kates J, Salganicoff A, Health and Access to Care and Coverage for Lesbian, Gay, Bisexual, and Transgender Individuals in the
U.S., Kaiser Family Foundation, January 2014; Cray A, Baker K, How the Affordable Care Act Helps the LGBT Community, Center for American Progress, May 2013.
7. IRS RECOGNITION
OF LEGALLY
MARRIED SAME-
SEX COUPLES
SAME-SEX
SPOUSAL
BENEFITS IN
FEDERAL
PROGRAMS
ACA COVERAGE
EXPANSIONS &
LEGALLY
MARRIED SAME-
SEX COUPLES
OTHER
CHANGES
•This is an example text.
Go ahead an replace it
with your own text. This is
an example text.
• Go ahead and replace it
with your own text.
•This is an example text.
Go ahead and replace it
with your own text
Implications of DOMA Decision & Other Policy Changes for
LGBT Health Care Access
8. Provision Issues to Consider
• Recognizes legally married same
sex couples which affects a
number of health-related
financial issues (e.g., spousal
health benefits now non-taxable
income for same sex couples)
• Requires all ERISA plans to
include legally married same-sex
couples in definition of “spouse”
and “marriage,” for purposes of
COBRA and other dependent
benefits
• Based on “state of celebration,”
regardless of whether couple lives
in state that recognizes same-sex
marriage
• But access to spousal coverage still
governed by patchwork of state-
policy and law. Majority of states
still impose bans on same-sex
marriages and do not recognize
same-sex marriages conducted
legally in other states. Employers in
these states not required to offer
coverage
DOMA Decision - Implications
IRS
Recognition
of Married
Same-Sex
Couples
NOTES: ERISA = Employee Retirement Income Security Act of 1974, a federal law that sets minimum standards for most voluntarily established pension and
health plans in private industry to provide protection for individuals in these plans; COBRA= Consolidated Omnibus Budget Reconciliation Act, an amendment to
ERISA, which provides some workers and their families with the right to continue health coverage for a limited time after certain events, such as the loss of a job.
SOURCES: Ranji U, Beamesderfer A, Kates J, Salganicoff A, Health and Access to Care and Coverage for Lesbian, Gay, Bisexual, and Transgender Individuals in the
U.S., Kaiser Family Foundation, January 2014; Cray A, Baker K, How the Affordable Care Act Helps the LGBT Community, Center for American Progress, May 2013.
9. Figure 8
NOTE: Under the ACA and Supreme Court DOMA ruling, states that recognize same-sex marriages required to provide insurance parity to same-sex couples.
Nevada- No Insurance Requirement, Insurance Coverage is the same as opposite-sex spouses, except for group health insurance benefits. Wisconsin- No
insurance requirement, but have limited spousal rights.
SOURCES: Ranji U, Beamesderfer A, Kates J, Salganicoff A, Health and Access to Care and Coverage for Lesbian, Gay, Bisexual, and Transgender Individuals in
the U.S., Kaiser Family Foundation, January 2014 (see issue brief for detailed list of data sources).
Relationship Recognition & Insurance Coverage Policies
for Same-Sex Partners, by State
AZ
AR
MS
LA
WA
MN
ND
WY
ID
UT
CO
OR
NV
CA
MT
IA
WI
MI
NE
SD
ME
MOKS
OHIN
NY
KY
TN
NC
NH
MA
VT
PA
VA
WV
CT
NJ
DE
MD
RI
HI
DC
AK
SC
NM
OK
GA
TX
IL
FL
AL
Civil union or domestic partner recognition AND requires insurance coverage, Same as Opposite-Sex Spouses (2 states)
State law banning same sex marriage and no law requiring insurance coverage for same-sex partners (29 states)
Same sex marriage legal AND requires insurance coverage, Same as Opposite-Sex Spouses (17 states + DC)
Civil union or domestic partner recognition BUT no insurance coverage requirement ( 2 states)
10. • Legally married same-sex federal
employees have same eligibility
for dependent spousal health
coverage and other dependent
benefits in Federal Employees
Health Benefits Program (FEHBP)
• Extends Family Medical Leave
Act (FMLA) workplace
protections to legally married
same sex couples, allowing time
off to care for a family member in
event of illness or birth of a child
• Based on “state of celebration,”
regardless of whether or not couple
lives in a state that recognizes same-
sex marriage
• But does not apply to state programs
or state employees (unless state
recognizes same sex marriage, civil
unions, or has other protections)
Provision Issues to Consider
DOMA Decision - Implications, continued
Same-sex
spousal
benefits in
federal
programs
SOURCES: Ranji U, Beamesderfer A, Kates J, Salganicoff A, Health and Access to Care and Coverage for Lesbian, Gay, Bisexual, and Transgender Individuals in the
U.S., Kaiser Family Foundation, January 2014; Cray A, Baker K, How the Affordable Care Act Helps the LGBT Community, Center for American Progress, May 2013.
11. • Marketplaces: Insurance plans in
health care marketplaces must
recognize legally married same-
sex couples for purposes of
determining tax credit eligibility
• Medicaid: Federal government
encouraging states to recognize
same-sex marriages for purposes
of determining Medicaid income
eligibility; states make ultimate
determination
Provision Issues to Consider
DOMA Decision - Implications, continued
ACA Coverage
& Legally
Married
Same-Sex
Couples
• Medicaid: No state has yet
submitted a State Plan Amendment
(SPA) for or against recognition of
same-sex spouses for
Medicaid/CHIP purposes
SOURCES: Ranji U, Beamesderfer A, Kates J, Salganicoff A, Health and Access to Care and Coverage for Lesbian, Gay, Bisexual, and Transgender Individuals in the
U.S., Kaiser Family Foundation, January 2014; Cray A, Baker K, How the Affordable Care Act Helps the LGBT Community, Center for American Progress, May 2013.
12. • Federal regulations require
hospitals participating in
Medicare and Medicaid (virtually
all in U.S.) to adopt written
policies and procedures
regarding patient’s right to visit
same-sex partner and must
prohibit discrimination based on
SOGI
• Federal regulations require long-
term care facilities, such as
nursing homes, to allow same-
sex spouses and domestic
partners to visit residents
• Health care proxy and advance
care directive provisions for
LGBT individuals
Provision Issues to Consider
Other Policy Changes
Other
Changes
• Enforcement still remains
challenge
SOURCES: Ranji U, Beamesderfer A, Kates J, Salganicoff A, Health and Access to Care and Coverage for Lesbian, Gay, Bisexual, and Transgender Individuals in the
U.S., Kaiser Family Foundation, January 2014; Cray A, Baker K, How the Affordable Care Act Helps the LGBT Community, Center for American Progress, May 2013.