2. • Largest lobe of liver(L)
at the left side and her
stomach(G) and
spleen(S) at the right
side, which is regarded
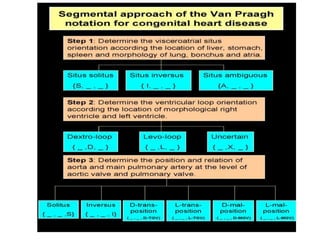
as situs inversus, {_, _,I}
3. • transverse liver and
right side
stomach(white arrow).
No definite spleen can
be found in the
abdomen. Situs
ambiguous is suspected
and {A,_,_} is assigned.
4.
5.
6.
7. • Normal pulmonary sideness of
broncho-pulmonary
anatomy,{S,_,_}: (1)
Hyparterial position of left
main bronchus and eparterial
position of right main
bronchus(black arrow: right
main pulmonary artery; black
dashed arrow: left main
pulmonary artery). (2)
Proximal take-off of the right
upper lobe bronchus(white
arrow) and distal take-off of
the left upper lobe
bronchus(white dashed
arrow).
8. • hyparterial location of
right main bronchus with
distal take-off of the right
upper lobe
bronchus(arrowhead). On
the other hand, the left
upper lobe bronchus
takes off from a relative
proximal location(white
arrow). These findings
also confirm situs
inversus.
9. • Eparterial location of
bilateral main bronchi
with proximal take-off
of the bilateral upper
lobe bronchi. Bilateral
right sideness of
broncho-pulmonary
anatomy is confirmed,
and splenic syndrome is
considered.
10. • hyparterial location of
bilateral main bronchi
with relative distal take-
off of bilateral upper lobe
bronchi. Bilateral left
sideness of broncho-
pulmonary anatomy is
observed, as combined
with multiple lobes of
spleen polysplenic
syndrome is considered
and {A,_,_} is assigned.
11. Rt atrial App left atrial Appendge
Typical appearance of left atrial
appendage(white arrow): tubular,
fingerlike shape, narrower than
right atrial appendage.
14. • morphological right
ventricle(mRV) located
leftward of the
morphologic left
ventricle(mLV), a L-loop
ventricular orientation as
the loop rule predicts,
assigned as {_,L,_}. Notice
thick moderator
band(black arrow)
extending from
ventricular wall to
septum.
16. • In morphological right
ventricle, the trabeculae are
coarse(white arrow) and the
papillary muscles(black arrow)
attach to both free wall and
interventricular septum. In
contrast, the papillary muscles
in morphological left ventricle
attach to free wall only. The
morphological left ventricle
has fine and thin with smooth
septal surface(S) as compared
with thick and coarse
trabeculae in morphological
right ventricle.
17. • aorta(A) arising from
morphological right
ventricle(mRV) and
pulmonary atresia. The
aortic root(white arrow)
locates anterior and
rightward of the
pulmonary trunk(PA),
which is designated as
"{_,_,D-TGA}"
18. • Aortic root(A) locates
anterior and leftward to
the main pulmonary
trunk(PA). This is
assigned as "{_,_,L-
TGA}".
19. • double outlet right
ventricle has aortic
root(A) and main
pulmonary trunk(PA)
arising in a parallel
plane with aorta at right
side and main
pulmonary trunk at left
side, which is
designated as {_, _, D-
MGA}.
20. • double outlet right
ventricle has aortic
root(A) and main
pulmonary trunk(PA)
arising in a parallele
plane from
morphological right
ventricle(mRV), which
has thick and coarse
trabeculae.
21. • double outlet left
ventricle has aortic
root(A) and main
pulmonary trunk(PA)
arising in a parallele
plane with aorta at left
side and main
pulmonary trunk at
right side, which is
designated as {_, _, L-
MGA}.
22. • double outlet left V has
aortic root(A) and main
pulmonary trunk(PA)
arising in a parallel
plane and both from
morphological left
ventricle(mLV).
34. Simple in 2/3 Complex in 1/3
PDA in 66%
VSD in 30%
ASD in 50%
VSD usually big or and multiple at any position
PS in 30% of those with VSD ( 10% 0f those with dTGV
usually due to
dynamic septal bulge into LV ( high RV pressure as it is
the systemic ventricle
Leftward malposition of infudubilar septum
valvular PS
Abnormal attachment of the mitral valve to VS
LV out flow tract
fibrous continuity between pulmonary valve and mitral valve
Sub aortic conus
Amount of Left to right shunt = Effective systemic flow
R to L = Effective Pulmonary flow
35. Early Pulmonary Vaso Occlusive disease Why
Big shunts ,
Hypoxia ,
Broncho-pulmonary collaterals carring desaturated blood to
preca-pillary pulmonary spaces >>>> sudden drop of oxygen
saturation in area with high saturation( excess reaction to
hypoxia)
Perianal flow to rt lung >>> thrombosis in the Left Lung
36.
37. • PFO or ASD
alone
• PFO or ASD +
PS
• PFO Or ASD +
VSD with No PS
(RV to LV & LA
to RA)
• PFO or ASD +
VSD +PS ( LV to
RV & RA to LA )
• PFO or ASD +
PDA ( Ao to PA
“right to left as
Ao carry
unsaturated
blood “&Left
atrium to Rt
atrium )
38.
39. RV Heave Or Hyperdynamic precordium No murmur VSD murmur PS murmur
Mur mur out of propation to the degree of cyanosis
40. • ASD >> No murmur splitting of S2 or single, RV
pulsation
• VSD >>>HF Systolic murmur , hyperdynamic
precordium
• VSD + PS two murmur out of portion of
degree of cyanosis
• PDA + PHT pink LL with cyanosis in upper limb
41. TGV with VSD
• Narrow Pedicle
• Absent Pulmonary
segement
• Pulmoary plethora
• Egg on side
42.
43.
44. ECG
• Upright T in V1 V2 after 3 days
• Right Ventricular hypertrophy
• Left Ventricular In cases with PVOD
PS
Big VSD
45. Role of echo
• Diagnosis PLA PA from LV
PSA Two circle Ao ant to Rt
sub costal LV >> PA RV >> Aorta
Shunt ASD PDA VSD
PS LV outflow obstruction
Coronary anomalies
46. • PSLA shows a patient with
transposition of the great
arteries and ventricular
septal defect. The
pulmonary artery arises
from the posterior (left)
ventricular, dives
posteriorly, and bifurcates
immediately into left and
right branch pulmonary
arteries. A large ventricular
septal defect is present in
the outlet septum.
49. • subcostal view shows
the left ventricle giving
rise to a vessel that
bifurcates, which is thus
identified as the
pulmonary artery
50. • subcostal view shows
discordant
ventriculoarterial
connections together
with the presence of
parallel, rather than
crossing, great arteries
arising from the
ventricles.
51.
52.
53.
54.
55.
56. • This right ventricular
angiogram shows a
patient with
transposition of the
great arteries. The aorta
arises directly from the
right-sided anterior
right ventricle (10° left
anterior oblique [LAO]).
57. • right ventricular
angiogram shows a
patient with
transposition of the
great arteries. The aorta
arises directly from the
right-sided anterior
right ventricle (70° left
anterior oblique [LAO]).
58. • left ventricular
angiogram shows a
patient with
transposition of the
great arteries. The
pulmonary artery arises
directly from the left-
sided posterior left
ventricle (30° right
anterior oblique [RAO]).
59. • left ventricular
angiogram shows a
patient with
transposition of the
great arteries. The
pulmonary artery arises
directly from the left-
sided posterior left
ventricle (20° cranial).
60. Natural History
• Death in 1st month in
50% and in One year
90% will die
• Live Longer if Wide ASD
with good mixing ,
surgery, PVOD, VSD and
PS
• Cyanosis Increase due
closure of shunts ,
growth , sub valvular
Pulmoary stenosis
• PVOD early Why
in those with Big VSD or
duct and in 10% in those
with without
HF later in the first month
Pink LL with upper limb
cyanosis in TGV with PDA
and PHTN
61. Emergency Treatment
PG
BALLOON ATRIAL SEPTOSTOMY if below 3 w
Decrease Atrial pressure
Increase O2
Echo wide ASD
If not or >3Ws>>>>>>>Blade Atrial septosotmy If still but
with wide ASD>>>>>>>>Surgical removal of Atrial
septum
Shunt
Pul Banding
Ligation of PDA+ creation of ASD
62. Simple TGA
• ASO if >2w
• MISSEDEARLY Aso .>>>>2
STAGES ASO
• CA abnormality>>>Atrial
swtich
63. With PDA
• Small>>> ASO
• Big Ligation + ASO or
Ligation + Creation of ASD
PS
Mild >>>>ASO
Significant >>>>ATRIAL Swtich + Pulmonary
surgery
64. VSD
Without PS
Small>>>>>>> ASO
Large>>>> ASO + Surgical VSD closure(2W_2M )
Atrial Switch + Surgical VSD closure( 3_4M )
Multiple or not amnable to closure>>>PA BANDING
With PS >>>>> Shunt Then Rastelle(4-5 Y)Or Lecomptete ( 1-2 Y)(
no conduit needed)
With subaortic stenosis >>>>>>Damus (1=2 Y )
69. • Both the Mustard and
Senning repairs create a
baffle within the atria
that redirects the caval
blood to the mitral
valve and the
pulmonary venous
blood to the tricuspid
valve.
72. The original description of the Mustard
technique (surgeon’s view). (A) The
patient is placed on cardiopulmonary
bypass and the right atrium is opened.
The atrial septum is excised, exposing
the pulmonary veins, which are now
visualized through the atrial septal
defect. (B) A pantaloon-shaped patch is
fashioned from autologous pericardium.
Attachment of the surgical patch is
begun to the left of the entrance of the
left pulmonary veins. (C) The pantaloon
baffle attachment is completed directing
the pulmonary venous blood to the
tricuspid valve, and directing the
superior and inferior vena caval blood to
the mitral valve. Mustard WT (1964)
Successful two-stage correction of the
transposition of the great vessels.
Surgery 55: 469–472.
75. • CMR offers quantification
of systemic RV function
and should be used
routinely unless there are
contraindications.
• Late gadolinium
enhancement can identify
areas of myocardial scar
that are associated with
adverse clinical markers
including atrial
arrhythmia.
79. Survival pattern after atrial switch
Concern:
The Rt.. Vent. is acting as a systemic vent.
Ultimately will fail with TR , AR
Arrhythmia ( mainly atrial )
Others:
SVC & IVC obstruction ( 5 - 10 % )
PV obstruction
Baffle leak (15 %)
Progressive Pul. Vascular disease (5 - 10 % ) this
is usually secondary to late operation or leak
Thrombotic complication
80. Clinical presentation:
CHF
TR ( 10 - 40 % )
Cyanosis (due to buffel leak)
Palpitation and syncope
Sudden cardiac death ( 5 %)
Atrial arrhythmia
RV dysfunction
Pul. HTN
81. Arrhythmia:
Late death is 4 time more in those with AF
than those without
Increase with time
Poorly tolerated
More dangerous in the presence of Rt. Vent.
Dysfunction
Caused by SA nodal damage and atrial scar
Junctional rhythm after Mustared operation
82. Atrial flutter with slow ventricular rate in a 25 years old
male after Mustard operation
83. • Electrocardiogram
in a patient with
transposition of
the great arteries
following atrial-
level repair. Note
the resting
bradycardia with
junctional rhythm
alternating with
slow sinus rhythm
and presence of
right ventricular
hypertrophy.
85. • The development of significant sinus bradycardia, while often
asymptomatic, is important to identify, because it will
influence and limit treatment with antiarrhythmic
medications
• Sustained intra-atrial reentrant tachycardia is a potential
cause of SCD in adults who have undergone atrial switch and
puts patients at risk for thromboembolism.
86. Treatment:
• Pacemaker for symptomatic bradycardia
• should be done by a person who have experience in navigating the
baffles to implant and sure the ventricular lead in the morphological
left ventricle
• Antiarrhythmic drug is not a good option
• Ablation. Atrial arrhythmias predominantly involve tissue of right atrial origin
which, because of the surgical anatomy, is found primarily in the pulmonary
venous atrium, making access for catheter ablation challenging.
• Although there are no data demonstrating that maintenance of sinus
rhythm prevents SCD, there is evidence that atrial arrhythmias
preceded or coexisted with VT in 50% of cases, suggesting that atrial
arrhythmias are a common trigger for ventricular arrhythmias
87. Figure 8 Chest radiograph of a patient with transposition of the great arteries and
atrial-level repair and following implantation of a dual chamber pacemaker
Love BA et al. (2008) Evaluation and management of the adult patient with transposition of the great arteries following
atrial-level (Senning or Mustard) repair
Nat Clin Pract Cardiovasc Med doi:10.1038/ncpcardio1252
88. • 27 y o. male with
transposition of the great
arteries was treated with
a Mustard procedure at
age ... Since that time he
had experienced SVT and
a permanent pacemaker
was placed. Note the
narrowness of the "aortic
knob" and the lack of the
pulmonary artery
segment on the PA x ray.
92. RV dysfunction with or without tricuspid
insufficiency may develop in 15% of patients in their
second and third decades of life
Severe tricuspid insufficiency may be addressed with
tricuspid valve repair or replacement if the RV
function is reasonably preserved. In cases with
severe failure, double switch operation with
retraining the left ventricle and heart transplant are
available options
93. • Transthoracic echocardiogram
(parasternal short-axis view) in
a patient with transposition of
the great arteries following
atrial level repair. Note the
ventricular septum (asterisk)
bowing away from the RV
towards the LV. Abnormal
septal configuration may
contribute to tricuspid
regurgitation, since the bowed
septum pulls the septal leaflet
away leading to a failure of
coaptation. LV = left ventricle;
RV = right ventricle.
94. Baffle leaks: Baffle leaks are usually small and not
hemodynamically significant and are best detected
by selective vena caval cineangiography.
Indication for intervention are significant left to
right shunt (Qp:Qs
>1.5:1), right to left shunt
Transcatheter device closure is preferable to surgical
closure
95. • Baffle leaks should be sought because they are
common and may alter treatment considerations such
as thromboembolic concerns or options for closure
• Echocardiography using agitated saline contrast is a
sensitive method for this assessment In some patients,
injection in upper and lower extremities may be
necessary to evaluate superior and/or inferior systemic
venous baffle leak, respectively, because a negative
study from an injection in upper extremity may not
exclude an inferior systemic venous baffle leak.
96. Baffle obstructions
may develop in 10% of patients .
Systemic venous obstruction is more common than
pulmonary venous obstruction and superior vena
caval (SVC)obstruction is more frequent than
inferior vena caval stenosis
Symptoms such as upper body edema indicative of
SVC syndrome are rare and are usually detected by
echo-Doppler studies, angiography or MRI
Balloon angioplasty of stenosed baffle obstruction) is
often successful; however long-segment obstructions
would require stents
98. Figure 6 Superior baffle-limb stenosis in a patient with transposition of the great
arteries after atrial-level repair and following implantation of a single-chamber
pacemaker
Love BA et al. (2008) Evaluation and management of the adult patient with transposition of the great arteries following
atrial-level (Senning or Mustard) repair
Nat Clin Pract Cardiovasc Med doi:10.1038/ncpcardio1252
99.
100. Selected cineangiographic
frame from inferior vena
cava (IVC)
injection in right anterior
oblique view
demonstrating stenosis
(arrows) of the
IVC baffle (A - PRE) in a
patient who had Mustard
procedure several years
previously. Following
balloon angioplasty (B -
POST), the narrowed
segment
improved (arrows). C,
catheter; LV left ventricle;
PA, pulmonary artery; SVA,
systemic venous atrium.
101. Selected cineangiographic
frame from superior vena
cava (SVC)
injection in posterio-
anterior view
demonstrating severe, long
segment
stenosis (arrow) of the SVC
baffle (a - PRE) in a patient
who had Mustard
procedure in the past.
Following stent (arrow)
implantation (b - STENT),
the
narrowed segment
improved (c - POST). SVA,
systemic venous atrium
102. Re- operation:
TR (repair or replacement)
AR ( Ao. Valve replacement )
Any Rt. - Lt. Shunt or Lt.. - Rt.
Shunt > 1.5
Surgery for arrhythmia
SVC & IVC obstruction - Balloon
Sever HF - Cardiac transplantation
Atrial change to arterial switch
103.
104.
105. Medical therapy for systolic ventricular dysfunction remains largely
uncertain
• Are outcomes improved with angiotensin-converting enzyme inhibitors,
angiotensin-receptor blockers, beta blockers, or aldosterone antagonists alone
or in combination in patients with a systemic right ventricle?”
• Although no clear benefit has been demonstrated for HF medical therapy
overall, there is speculation of benefit in more symptomatic patients or those
with larger and or more dysfunctional right ventricles.
• Concerns regarding routine use of beta blockers for asymptomatic RV
dysfunction include potentially greater predisposition to bradycardia and
limited distensibility of the interatrial baffle,which creates a preload limited
physiology.
.
106. • Patients with dysfunction of the systemic right ventricle are at
risk of developing ventricular arrhythmias. The role of ICD
implantation for primary prevention of arrhythmia in patients
with a low systemic ventricular ejection fraction is uncertain
113. • LV Must be prepreared
• NO Sig Ao or Pul obstruction
• Suitable coronary anatomy
• 2 stage Arterial switch
PA banding untill PA P > 75 % of systemic
pressure
Then arterial switch
114. Arterial switch
• little data concern long term follow up. The aim is to decrease
arrhythmia and preventing RV from acting as systemic Vent.
• Coronary abnormalities are common after arterial switch (6% to
10%), especially in the setting of coronary anomalies at birth, or extensive
manipulation of the coronaries at the time of the operation. Most
coronary problems tend to occur in childhood in the first few years after
surgery, with limited experience in adults,
• long-term natural history of the coronary arteries after arterial
switch is still unknown. This is particularly true regarding the impact of
risks for concomitant acquired coronary artery disease in patients whose
coronary substrate is not normal.
• Coronary ostial stenosis late after arterial switch may be repaired by
coronary artery bypass graft surgery or ostial arterioplasty techniques
•
•
115. • New pul. A. kinking and branch pulmonary artery stenosis may be seen;
when these are severe, transcatheter (balloon angioplasty or stent) or
surgical therapy may become necessary.
• PS affects 5% to 15% of patients after arterial switch and may occur
anywhere in the pulmonary tree including the pulmonary valve, main PA,
and branch pulmonary arteries. Interventional decisions should be guided
by a combination of symptoms and severity of stenosis.
• Severe RVOT obstruction not amenable or responsive to percutaneous
treatment is an indication for reoperation; lesser degrees of obstruction
can be considered an indication for intervention if greater degrees of
exercise are desired.
• Pulmonary valve replacement or repair is often considered when severe
PR is present and there is significant RV dilation or RV dysfunction.
116. • Dilation of the neoaortic root with preserved aortic valve
competence. The threshold aortic diameter at which
dissection/rupture risk exceeds the risk of operation is not
known, and consequently the threshold for prophylactic
operation for neoaortic root dilation is undefined.
• Severe aortic insufficiency is seen in less than 1% of the
patients Although some degree of neoaortic valve
regurgitation is common, surgery to replace the neoaortic
valve has only rarely been reported
• aorta obstruction when severe, transcatheter (balloon
angioplasty or stent) or surgical therapy may become
necessary
117.
118.
119. Rasstelle
• RV to PA valuated
conduit
• Closure of VSD with LV
- aorta Tunnel
120. • Rastelli Repair for
Transposition of the Great
Arteries 1. Right ventricle to
pulmonary artery conduit 2.
Intracardiac left ventricular to
aortic tunnel 3. Transposition
of the great arteries
Postoperative right ventricle to
pulmonary artery conduit and
intracardiac left ventricular to
aortic tunnel (Rastelli repair)
for: Transposition of the great
arteries Ventricular septal
defect Pulmonary stenosis
• 1
122. • figure shows the
innovations of the REV
procedure relative to
the Rastelli procedure,
with resection of the
muscular outlet septum
(B) and use of Lecompte
manoeuvre (C) which
avoids the use of an
extacardiac conduit.
123. Concern
• Long term considerations after the Rastelli
operation include:
• 1. Right ventricle–to-PA conduit dysfunction
(Section
• VSD patch leaks/dehiscence
• 3. LV-to-aorta internal baffle stenosis
• 4. Scar-based VT
126. Corrected TGV
SLL or IDD
• VSD 80%
• Left Side AV VALVE
REGURGITATION 30%
• Seventy percent to 90% of
patients with CCTGA have a
dysplastic or Ebsteinlike
malformation of the tricuspid
valve TR is often because of a
dysplastic tricuspid valve and has
been shown to be an
independent predictor of death in
CCTGA
• Pulmonary stenosis 50%
• Arrhytmia and HB
• Dextro cardia in 50%
127. • Coronary artery mirror
image
• RCA gives LAD and CX
Left >>>RT coronary
course
• Conductive system
inversion so septal
activation from Rt to Lt
128.
129.
130. Conduction system In
CTGA
• Dual AV nodes and inversion of AV
bundles.
• Increasing incidence of AV block, at a
rate of approximately 2% per year,
• An anterior and right-sided AV node
that was situated anterolateral to
the mitral-pulmonary valve junction.
This node connects to the
morphologic (right-sided) LV by a
descending bundle of conducting
tissue that travels anterior and
lateral to the pulmonary outflow
tract. Hiss bundle travels Long
distance between AVN and Base of
VS and is subjected significant
excurtion during mitral valve closure
• Many ccTGA patients also have a
posteriorly-situated AV node, which
is often hypoplastic, in addition to a
functional anterior node.
131.
132. • The bundle branches are inverted, each typical
of the morphologic ventricle they serve.
• In the presence of a subpulmonary VSD the
descending AV bundle is located on the
anterosuperior and anteroinferior borders of
the defect. This is in contrast to concordant
hearts {S,D,S} in which the conduction bundle
travels along the posteroinferior margin of the
VSD.
133.
134.
135. Clinical presentation
• Depends on associated Lesion and Function of the
anatomical RV that support systemic circulation
• SOB HF CYANOSIS Heart Block SD Conduction
abnormalities are common, and the prevalence of
spontaneous complete heart block increases with age.
• Single loud S2 at 2nd left space mimks Pulmonary
hypertension
• PS heard at aortic area ( Rt St Border)
• Murmur of Left side AV regurgitation usually heard at
LSB
136. X ray
• Straight left border of the heart
• Narrow Pedicle
• Absent Pulmonary segment
137. • anteroposterior chest
radiograph revealing
the straightened left
heart border formed by
the aorta, which is more
leftward and anterior
than usual.
138. The upper part of cardiac silhouette
as seen in the chest radiograph
appears abnormally straight because
of the loss of the normal arterial
relationships.
142. • characteristic features of
corrected transposition Q waves
in III, in aVF, and in the right
precordial leads. T inversion in V5
V6 upright inV1
• HB and arrhythmias
146. ECHO
• Septum can not be seen in Lp view (septum
parallel to Beam
• Ao arise from anatomically RV
• PA from anatomical LV
• LV to Rt RA open into MV
• LA open into TV ( Rt TV 0
• Ao ant ant to Left
• Associated Lesions
147. • A transthoracic
echocardiogram in the
apical 4-chamber view
illustrating the
moderator band in the
left-sided ventricle and
the apically displaced
left atrioventricular
valve suggesting that it
is the morphologic right
ventricle.
149. • transthoracic
echocardiogram in the
parasternal short axis
view demonstrating the
anterior and leftward
aorta. The left coronary
artery can be observed
at the 10-o'clock
position.
150. • The systemic RV is
severely
hypertrophied, is
filled from the left
atrium (LA), and
ejects into the aorta
(Ao). The RV outflow
tract (asterisk) is
severely narrowed
by a muscle bridge
(arrowhead), most
markedly during
systole.
151.
152. • Subcostal view of a 1-
year-old child with L-
transposition of the great
arteries, valvular and
subvalvular pulmonic
stenosis, and a moderate
outlet ventriculoseptal
defect (VSD). Note the
ventriculoarterial
discordance. Note the
posterior, rightward
position of the pulmonary
artery.
153. image depicting the position
of aorta and pulmonary
artery in D-TGA.
Image depicting the position
of aorta and pulmonary artery
in L-TG
157. Figure 2. Transesophageal echocardiographic images.
Orchard E A et al. Circulation. 2010;122:e441-e444
. Transesophageal
echocardiographic images.
Transesophageal images at early
systole (A), late systole (B), and
diastole (C). The RV outflow tract
(asterisk) is narrowed most
severely during mid and late
systole. LA indicates left atrium; Ao,
aorta.
158. • Doppler echocardiography showing
an anatomic right ventricle located to
the left. Note the greater
trabeculation and hypertrophy than
in the anatomic left ventricle, the
presence of a moderating band (red
arrow), and the more apical
implantation of the septum valve of
the systemic atrioventricular valve (*)
in comparison to the anatomic left
atrioventricular, located at the right
in this case (**). The systemic
atrioventricular valve presents
eversion of one of the leaflets (white
arrow), which originates a severe
insufficiency jet. LA, left atrium; LV,
anatomic left ventricle; RA, right
atrium; RV, anatomic right ventricle.
159. • CMR is useful for
quantification of systemic
RV size and function.
Administration of
gadolinium contrast is
useful in identifying fibrotic
myocardium demonstrated
by late gadolinium
enhancement
160. TTT
• Asymptomatic >>> Search for associated
defects Follow up for Ventricular function
and Arrhythmia also may be BE prophylaxis
• Pallative
Shunt
Banding of PA
Corrective
VSD with good systemic ventricular function and
no significant TR>>>>
Surgical closure ( high Risk of HB )
VSD With PS with good systemic ventricular
function and no significant TR>>>> Closure +
conduit between LV and PA
VSD with impaired systemic ventricular function or
significant TR>>>>PA banding + VSD closure +
DOUBLE switch ( Sys Venous >>LA>>RV>>PA and
Puul Venous >>Rt Atrium >>LV >>AO
VSD + PS with impaired systemic ventricular
function or significant TR>>>Seening + Closure VSD
with tunnel between LV and Aorta + RV to PA conduit
Or Fontan
162. tricuspid valve replacement is preferred to tricuspid
repair in the adult CCTGA population.
Tricuspid valve repair has been attempted; however,
recurrent clinically significant TR is observed
frequently after repair
163. Adults with CCTGA and pulmonary atresia or
stenosis were often managed in childhood by placing
a conduit from the morphologic LV to the PA,and
progressive conduit dysfunction is common.
Conduit intervention or replacement will diminish
the pressure in the subpulmonic ventricle and may
result in ventricular septal shift toward the
subpulmonic left ventricle, including the septal
leaflet of the systemic tricuspid valve and thuscan
result in worsening of TR and a detrimental impact
on systemic RV function
164. VSD + PS with impaired systemic
ventricular function or significant
TR>>>Seening + Closure VSD with
tunnel between LV and Aorta + RV to
PA conduit
Or Fontan
165. • An anomalous second AVN is the functioning
one generaly located beneath the opening of
right atrial appendage at the lateral margin
between the pulmonary and mitral valves .It
has an anterior positionand gives immediately
to AV bundle underneath the pulmonary
valve.This accessory node may be hypoplastic
and not functioning
166.
167.
168.
169.
170.
171.
172. cTGV
• Apical image revealing
atrioventricular
discordance. Note the
pulmonary venous
return into the left
atrium, with sequential
flow through the
tricuspid valve to the
right ventricle. The right
ventricle is systemic
177. • aortic root(A) leftward
to the main pulmonary
trunk(white arrow).
According to the loop
rule, she would have L-
loop ventricular
orientation.
178. • Inversion of the great
vessels: the aortic
root(A) is located
posterior and rightward
to the main pulmonary
trunk(PA), at the level of
the valves, which is
designated as "{_,_,I}".
179. • Normal configuration of
the great vessels: the
aortic root(A) is located
posterior and leftward
to the main pulmonary
trunk(PA), at the level of
the valves, which is
designated as "{_,_,S}"
Editor's Notes
Figure 5. Necropsy specimens showing AV concordance (left) and AV discordance (C-TGA, right). The crux anatomy facilitates recognition of AV morphology because the tricuspid valve is always lower (arrow) than the mitral valve and always enters a morphological RV. Although the ventricular morphology may be suggested by the more trabeculated pattern of the RV, this is not always consistent or easily identified. Reproduced, with kind permission of Springer Science and Business Media, from Seward JB, Tajik AJ, Edwards WD, Hagler DJ. Two-Dimensional Echocardiographic Atlas, Vol 1: Congenital Heart Disease. New York, NY: Springer-Verlag; 1987.
Figure 1. Schematic drawings of the Mustard operation. A, An atrial baffle diverts blood from both the superior vena cava and the inferior vena cava across to the mitral valve and LV, which ejects blood to the pulmonary artery. B, The pulmonary venous blood is returned to the tricuspid valve and RV, which ejects blood into the aorta. IVC indicates inferior vena cava; LL, left lower pulmonary vein; LU, left upper pulmonary vein; MV, mitral valve; RL, right lower pulmonary vein; RU, right upper pulmonary vein; SVC, superior vena cava; and TV, tricuspid valve.
Figure 6. Chest radiographs of a patient with C-TGA and levocardia (A) and dextrocardia (B). A, The vascular pedicle on the left, where the usual rounded convexities of the descending aorta and pulmonary artery are seen in a normal heart, is unusually straight. In addition, the ventricular border has a “humped” appearance and is more vertical than usual. B, The apex of the heart points to the right, but the gastric bubble is on the left. This should always raise the suspicion of C-TGA because dextrocardia occurs in ≈20% of cases. The gross cardiomegaly is the result of profound heart failure secondary to severe AV valve regurgitation.
Figure 9. A, Chest radiograph of a 16-year-old young man with C-TGA just after implantation of an endocardial pacemaker. Reportedly, his ejection fraction was 40%, and he had moderate systemic AV valve regurgitation. B, Chest radiograph 18 months later at the time of referral. His systemic ventricular ejection fraction was 15%, and he had severe psystemic AV valve regurgitation. Cardiac transplantation was the only viable surgical option because referral was too late for conventional operation. Reproduced from Warnes64 with permission from the American college of Cardiology Foundation.
Figure 7. ECG of a patient with C-TGA. Septal activation occurs from right to left, and therefore Q waves are seen in the right precordial leads II and III, but no Q waves are seen in V5 and V6.
Figure 8. Apical 4-chamber view of a patient with C-TGA in the same tomographic plane as Figure 5. Pulmonary veins (dashed arrows) enter the left atrium (LA). The cardiac crux has a mirror-image appearance with the right-sided AV valve clearly inserting higher than the left-sided valve (arrows). The lower valve is the tricuspid valve, which enters the morphological RV, which has prominent trabeculations (arrowheads). AS indicates atrial septum; LV, morphological LV; and RA, right atrium. Reproduced, with kind permission of Springer Science and Business Media, from Seward JB, Tajik AJ, Edwards WD, Hagler DJ. Two-Dimensional Echocardiographic Atlas, Vol 1: Congenital Heart Disease. New York, NY: Springer-Verlag; 1987.
Figure 2. Transesophageal echocardiographic images. Transesophageal images at early systole (A), late systole (B), and diastole (C). The RV outflow tract (asterisk) is narrowed most severely during mid and late systole. LA indicates left atrium; Ao, aorta.
Figure 10. “Double-switch” operation for C-TGA using the Mustard atrial baffle technique and arterial switch procedure. The VSD has been closed with a patch. Venous blood from the superior and inferior vena cava (SVC, IVC) is directed to the RV and then to the pulmonary trunk, and pulmonary venous blood is directed to the LV and then to the aorta.
Figure 6. Transesophageal echocardiogram showing the aorta arising from left side of the right ventricular outflow tract.