Download to read offline






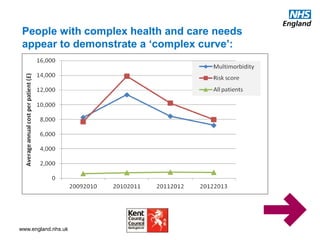





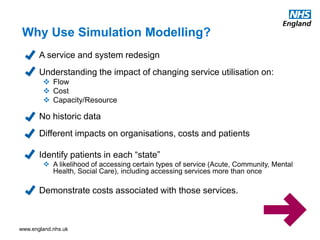










The document discusses the testing of integrated care service models for patients with complex care needs, aiming to improve their quality of life and experiences through person-centred, coordinated care. It highlights the importance of simulation modelling in advising and influencing care delivery, emphasizing the challenges of managing multi-morbidity and the need for personalized integrated care. The document outlines strategies for enhancing care coordination, addressing inequalities, and implementing effective commissioning and funding approaches within the NHS.






















































































