Downloaded 101 times






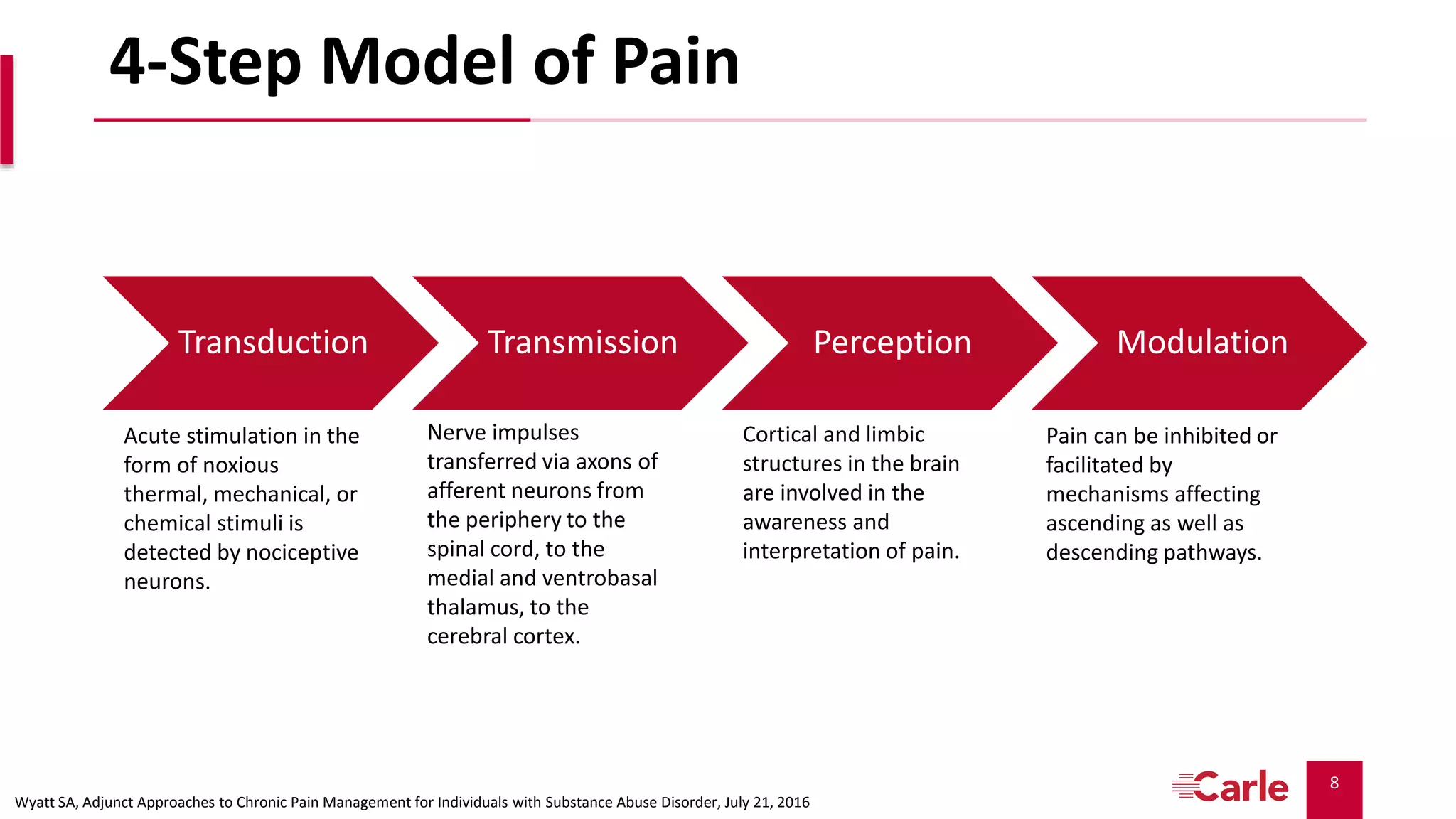







































The document discusses pain management in palliative care, outlining models and pathways for understanding pain, including its biochemical and neurohormonal mechanisms. It covers the use and complications of opioids, strategies for managing pain, nausea, and constipation, and explores case studies involving the complexities of patient care. Additionally, it highlights the importance of multidisciplinary approaches in treating pain and associated symptoms in patients with malignancies.























































































