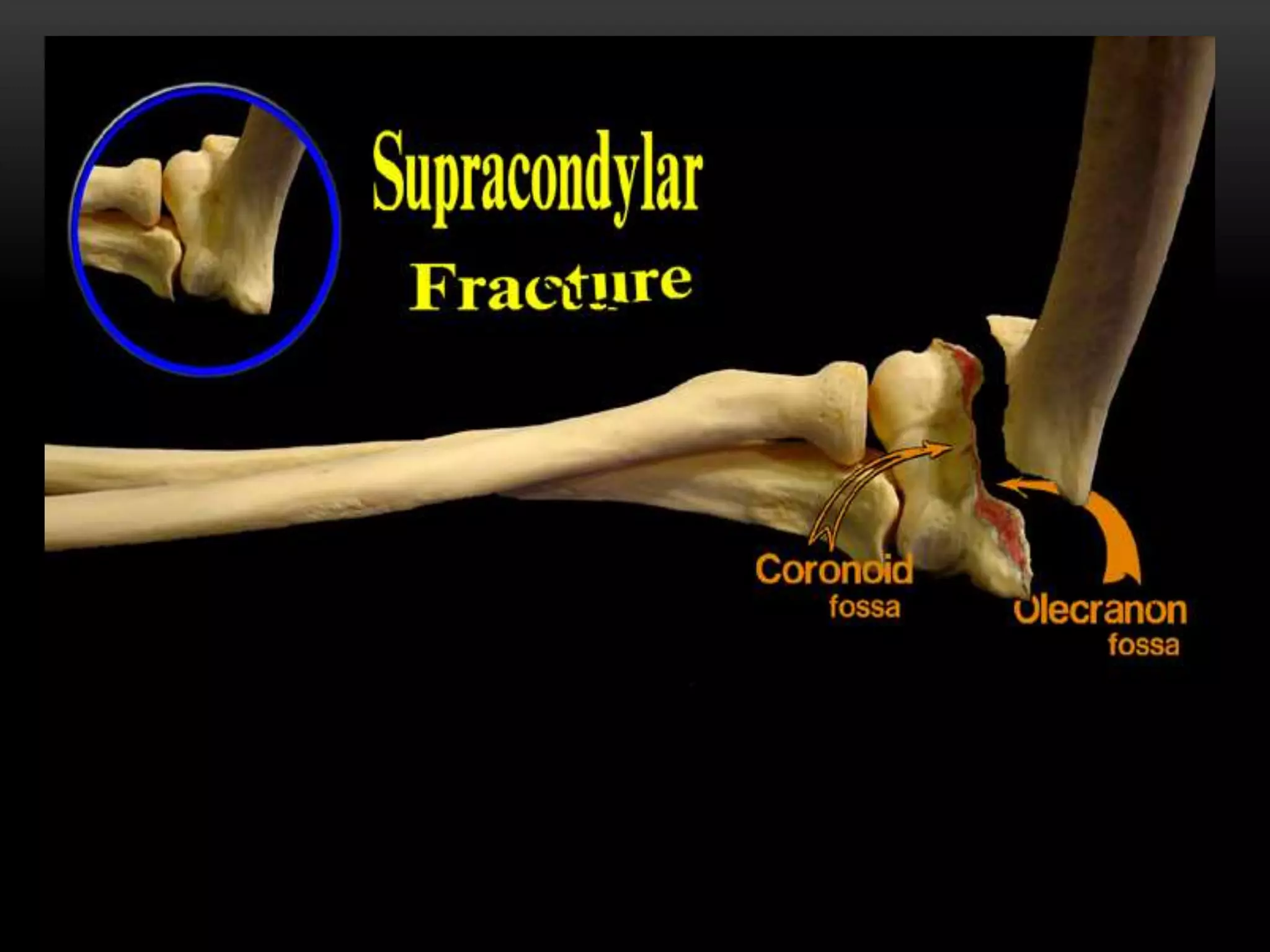
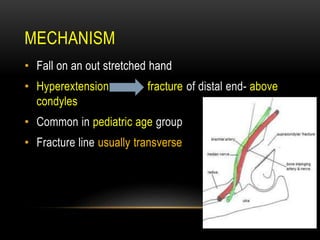
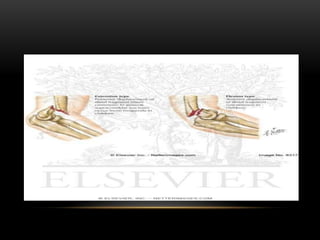
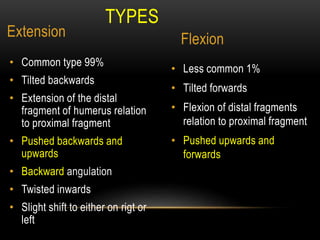
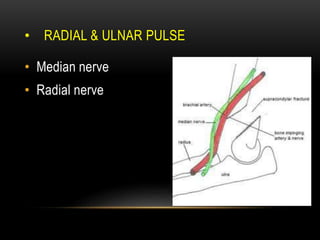
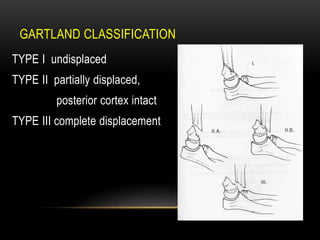
Supracondylar fractures of the humerus occur just above the elbow joint. They are most common in children and usually result from a fall onto an outstretched hand, causing hyperextension of the elbow. There are two main types - extension type fractures tilt the distal fragment backwards while flexion types tilt it forwards. Displacements can include posterior or medial shifting of the fragments. Treatment depends on the degree of displacement and may include closed reduction, percutaneous pinning, or open reduction and internal fixation. Complications can include nerve injuries, vascular injuries, malunion and contracture.