Downloaded 21 times

![Introduction
Suicide is one of the leading causes of death in prisons internationally, and
has been a source of major concern in the New Zealand correctional
environment for the last 20 years. It is one of the events that correctional
services regularly monitor a key performance indicator [see the annual reports
of the Chief Executive of the Department of Corrections for example]. Prison
suicides have resulted in significant public concern that has contributed to two
Department of Corrections reports into prison suicide [Department of
Corrections 1995, 1996] and one Ministerial Inquiry [Mason et al, 1988] that,
inter alia, addressed this concern.
All of this sits in the context of widespread societal concern regarding
escalating suicide rates during the 1980s and early 1990s, and a coordinated
attempt to reduce suicide rates, most especially youth and Maori suicide rates
which were increasing most rapidly. Like societal suicide rates more
generally, prison suicide rates and related policy and service responses show
that it is possible to both worsen and improve suicide rates by service and
policy intervention, but to what degree is difficult to define with certainty.
Nonetheless, problems with suicide in prison have brought about service
responses in the corrections and health sectors which have had positive
impact. This is a tale of 2 peaks, of vulnerable people, and service responses.
The New Zealand Correctional Environment.
As a country of 4.1 million people, we currently have a prison muster of
approximately 7500 prisoners [New Zealand Herald, 26/10/05], or 183
inmates per 100,000 population. In comparison, the United States has 680
per 100,000 ppn, but all other countries like us have fewer prisoners, Australia
having 110, England and Wales 125 and most of Western Europe less than
120 [Department of Corrections, 2004 a and 2004 b]. Prisoners are on
average young, with a mean age of just under 30, and half are of Maori
ethnicity.](https://image.slidesharecdn.com/file214-120518204018-phpapp02/85/Suicide-and-Suicidal-Behaviour-in-Prisons-2-320.jpg)

![imprisonment and suicidality. Add to that the experience of imprisonment and
the reasons for it, often involving major stress, withdrawal from drugs, entry
into a new and at times intimidating environment, and it makes the presence
of suicidality in inmates very likely.
If one adds to that the increased rate of mental illness amongst prisoners then
the co occurrence becomes unsurprising. There are multiple reasons why
inmates suffer more mental illness [Ogloff, 2002]. For instance, the causes
and precipitants of offending and mental illness overlap, for instance the role
of substance misuse in both. Second, mental illness may lessen people’s
capacity to cope, resulting in minor ‘disability’ related offending such as
disorderly behaviour and minor property crime, in people who are otherwise
homeless. Third, mentally ill people might be more easily caught, resulting in
an apparently greater incidence of offending, when it is more about detection.
Finally, policies or competencies of state agencies such as police, courts or
mental health services may favour people with mental illness being
incarcerated.
Whatever of these processes apply, increased prevalence of all the major
mental disorders amongst prisoners, but most particularly substance misuse,
major depression, post traumatic stress disorder, schizophrenia and
personality disorders is very well documented internationally [Fazel and
Danesh, 2002; Ogloff, 2002]. We performed a study of psychiatric morbidity in
NZ prisons in New Zealand in the late 1990s, and found very similar findings
[Simpson et al, 1999; Brinded et al, 2001; Simpson et al, 2003].
Suicide in New Zealand Prisons
Prior to 1980, I cannot find record that any more that 2 people died by suicide
in NZ prisons in any one year. Since then, there have only been 4 years when
there have been 2 or fewer [see figure 1]. Two discernable peaks in the
number of suicides can be seen, the first being in 1984 and 1985, and the
second in 1994 and 1995. In between these peaks, suicide numbers have not
sustainedly fallen to their pre 1980 levels, although population suicide rates](https://image.slidesharecdn.com/file214-120518204018-phpapp02/85/Suicide-and-Suicidal-Behaviour-in-Prisons-4-320.jpg)
![have fallen back to levels more typical of the early 1980s [Ministry of Health,
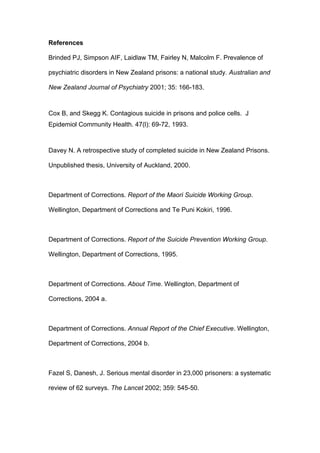
2005]]. Expressed a ratio of the prison muster, however, it appears that the
rate as a percentage of the average daily muster is static or falling as
musters have risen [Figure 2]. Why then have we had these 2 apparent
peaks, and what gave rise to them? Why have suicide rates not dropped
since back to the 1980 levels?
Over the time period 1986-1992, the rate of suicide by inmates was 2.5 -5.2
times that of the general population. This degree of increase is similar to other
nations internationally [Department of Corrections, 1995]. There appeared
however to be particular issues in relation to these 2 peaks. For instance,
Skegg and Cox [1991, 1993] found that there were particular clusters in space
and time of the suicides that occurred prior to 1990. It appeared that a suicide
increased the risk that others could suicide, suggesting that prisoners
represented a population at risk. One event might spark another.
Davey [2000] studied these 2 peaks and found significant differences between
the suicides in the 2 groups. Those who killed themselves prior to 1990 were
significantly older, were almost all sentenced prisoners, most had a history of
self harm and a history of mental illness. After 1990 they were much younger,
only about 1/3 had prior mental health involvement, most were on remand and
did not have a prior history of self harm. The majority were of Maori ethnicity
regardless of the time period. Why should the 2 groups of suicides be
otherwise so different?
The answers lie in public policy. In 1984 the Auckland Hospital Board stopped
admitting mentally ill prisoners from Auckland and Mt Eden Prisons. These
were sentenced prisoners with serious mental illness. As the Mason Inquiry
documented, 12 died by suicide in the period that followed [Mason et al,
1988]. They were older sentenced prisoners with a history of serious mental
illness who died because of a policy change by an agency of government. All
were Maori. These tragedies led to the establishment of the network of
forensic psychiatry services that exist around the country today. We have not](https://image.slidesharecdn.com/file214-120518204018-phpapp02/85/Suicide-and-Suicidal-Behaviour-in-Prisons-5-320.jpg)
![seen a similar peak of suicides of people with serious mental illness since
those services were established.
In the early 1990s, coinciding with the highest rates of societal offending,
suicide and unemployment, bail laws were tightened and there was a sudden
rise in the number of remand prisoners. And a new group of people became
predominant amongst the suicides in custody. They were young men on
remand, generally with no history of mental health contact or prior suicidality,
who found themselves in custody. These people comprised the early to mid
1990s peak in suicides in custody. The recognition of this group with new
needs led to a review of the policies and procedures of the Department of
Corrections [1995, 1996], the effect of which has been to hold, or perhaps
reduce, the rate of suicide amongst inmates.
Thus the lessons of these 2 peaks has been that both inmates with serious
mental illness and the young men with offending histories going through the
upheaval of imprisonment are at risk.
How Common is Suicidality amongst inmates?
In order to understand this better, we asked about suicidality in the National
Study on Psychiatric Morbidity in NZ Prisons [Simpson et al, 1999]. We
asked:
Since you have been in prison, have you at any time thought a lot about
death?
Since you have been in prison, have you at any time felt so low you thought a
lot about committing suicide?
Did you tell the prison nurse or doctor about feeling suicidal?
Did you make a plan as to how you might do it?
Since you have been in prison have you attempted suicide?
The answers we received are shown on Table 1. In short, about one fifth of
prisoners reported thinking significantly about suicide at some stage of their](https://image.slidesharecdn.com/file214-120518204018-phpapp02/85/Suicide-and-Suicidal-Behaviour-in-Prisons-6-320.jpg)
![imprisonment, confirming the finding of Skegg and Cox that this population
were at risk of suicide, and the cluster effects they found make sense in this
context. Interestingly, there was no difference in the prevalence of suicidal
ideation on the basis of age, gender or remand and sentenced status of the
inmate. However, Maori were less frequently responded that they thought a
lot about suicide [see Table 2]. Given that Maori are more likely to be the
victims of successful suicide in prison [Department of Corrections, 1996;
Davey, 2000] this suggests that the presence of suicidal thoughts maybe
more lethal amongst Maori than non-Maori inmates, and should be responded
to with greater concern [Simpson et al, 2003].
Service responses
Given that we have a history of experience that tells us that making rapid
changes in policy has very negative impact on offenders with a risk of suicide,
what lessons have been learned and still need to be learned? First, a public
health approach must be taken. The work of Skegg and Cox, and our work on
the prevalence of suicidal ideation, tells us that it is not discrete individuals
who are at risk of suicide, but a group of people, similarly at risk, who if they
have the availability of others modelling the behaviour, or the means and
opportunity to kill themselves, may take it. Thus processes like removing
hanging points and constructing prisons with few opportunities to kill oneself
are very important. Second, all prison staff need education and training in how
to assess and look for people at risk. Third, new prisoners should be screened
for suicidal feelings and referred for intervention from primary health staff if
thought to be at risk. All these steps have been taken by the Department of
Corrections [see Department of Corrections 1995, 2004b], and have almost
certainly contributed to the holding of the absolute number and proportionate
decline in suicide rates since 1995.
The other major service development is that of regional forensic services
providing secondary level CMHC like care to prison populations, including
transfer to inpatient facilities if needed. These services were commenced in
1989 after the Mason Inquiry and have developed since with a clear mandate](https://image.slidesharecdn.com/file214-120518204018-phpapp02/85/Suicide-and-Suicidal-Behaviour-in-Prisons-7-320.jpg)
![for the care of people with serious mentally illness within the correctional
system [Simpson and Chaplow, 2001; Ministry of Health, 2001]. In the main
successful, these services have the brief to provide multidisciplinary care
including acute assessment, follow up clinics, transfer to inpatient facilities if
needed and to arrange hand over of care upon release to the community.
They are looking to further develop the standard to care for some prisoners to
be closer to an assertive community treatment model. It is estimated that
between 10 and 15% of all inmates should be receiving assessment or
treatment from mental heath services [Brinded et al, 2001]. If one adds to this
the rising prison musters, it is clear that mental health services to prisons
need to be expanded in parallel.
We know from our prior work that only inmates with current bipolar disorder
regularly contact mental health services in prison, whilst fewer than 40% of
those with schizophrenia or major depression receive treatment in prison
[Simpson et al, 1999]. This suggests that the means we use to detect those
inmates with serious mental illness is missing many inmates. The current
process of screening new inmates for mental illness hasn’t been validated and
yet there are validated screening tools available internationally for this
purpose. But we don’t know whether they will work for in a New Zealand
context. A project is currently being planned to develop a validated tool for
New Zealand, as it is agreed between the Ministry of Health and the
Department of Corrections that screening all prisoners for mental illness and
suicidal risk is an important priority.
Conclusions
As can be seen, health and correctional policies have evolved dramatically
over the last 20 years, at times without thought for the mental well being and
risk of suicide of inmates. There is evidence that policy can get it wrong and
get it right in terms of developing services for these people, but there is need
for active and continual collaboration between the sectors if this group of
people at risk of self harm are not to manifest that risk. Current initiatives for
building prisons which incorporate architectural safety, providing awareness of](https://image.slidesharecdn.com/file214-120518204018-phpapp02/85/Suicide-and-Suicidal-Behaviour-in-Prisons-8-320.jpg)


![Simpson AIF and Chaplow DG. New Zealand model for the provision of
forensic psychiatry services. Psychiatric Services, 52:973-974, 2001.
Skegg K, Cox B. Suicide in custody: occurrence in Maori and non Maori New
Zealanders. New Zealand Medical Journal 1993; 106: 1-3.
Figure 1.
Prison Suicides and Average Daily Muster
7000 12
6000 10
5000 8
4000 Average Muster
6
3000 Number of Suicides
2000 4
1000 2
0 0
1980
1981
1982
1984
1986
1987
1989
1991
1992
1994
1996
1999
2000
2001
1983
1985
1988
1990
1993
1995
1997
1998
2002
Year
[Data derived from Department of Corrections, 1995, 2004b]](https://image.slidesharecdn.com/file214-120518204018-phpapp02/85/Suicide-and-Suicidal-Behaviour-in-Prisons-12-320.jpg)
![Figure 2.
Prison Suicide by Average Daily Muster
7000 0.35
6000 0.3
5000 0.25
% Suicides
4000 0.2
Muster
Average Muster
3000 0.15 % of average Muster
2000 0.1
1000 0.05
0 0
1980
1981
1982
1985
1986
1989
1990
1991
1992
1994
1995
1996
1997
1998
1999
2000
2001
2002
1983
1984
1987
1988
1993
Year
[Data derived from Department of Corrections, 1995, 2004b]](https://image.slidesharecdn.com/file214-120518204018-phpapp02/85/Suicide-and-Suicidal-Behaviour-in-Prisons-13-320.jpg)
![Table 1. Self Report of Suicidal Ideation or Behaviour since being in Prison
[n=1159; Simpson et al, 1999]
Present Not Present Percentage
Present
Thoughts of death 323 836 27.9
Thoughts of 238 921 20.5
suicide
Reported thoughts 80 1079 6.9
to doctor or nurse
Suicidal plans 52 1107 4.5
Suicidal attempts 30 1129 2.6](https://image.slidesharecdn.com/file214-120518204018-phpapp02/85/Suicide-and-Suicidal-Behaviour-in-Prisons-14-320.jpg)
![Table 2. Self report of Suicidal Ideation by Ethnic Group [n=1159, Simpson et
al, 1999]
A lot of Pakeha Maori Pacific Own Total
thoughts of Peoples specificatio
Suicide n or other
No 279 462 72 108 921
Yes 86 90 23 39 238
Percentage 23.6% 16.3% 24.2% 26.5 20.5%
suicidal](https://image.slidesharecdn.com/file214-120518204018-phpapp02/85/Suicide-and-Suicidal-Behaviour-in-Prisons-15-320.jpg)

This document summarizes patterns of suicidal behavior among inmates in New Zealand prisons over the past 20 years. There were two distinct peaks in prison suicides, in 1984-1985 and 1994-1995, which were influenced by changes in health and correctional policies. Screening tools and mental health services have since been developed and expanded for prisoners to help address suicide risk, though continued collaboration between health and corrections sectors is still needed.


































































































