INTRODUCTION
Substance related disorderis also known
as drug abuse or substance abuse is a patterned use of
a substance (drug) in which the user consumes the
subbstance in amounts or with methods which are
harmful to themselves or others.
Substance related drugs involves drugs
that directly activate The brain's reward system. The
activation of The reward system Typically causes feelings
of pleasure. The specific pleasurable feelings evoked
vary widely depending on the drug
3.
What is meanby drug?
A drug is defined as any
substance that when taken into the
living organism, may modify one or
More of its function - WHO
Substance related disorders are
composed of two groups...they are
• Substance use Disorders
• Substance induce disorder
ABUSE
To use wrongfullyor in a harmful way.
It is a pattern of physically hazardous
use of drug
DEPENDENCE
A Compulsive or chronic requirement.
The need is so strongly as to
generate distress( either physical or
psychological) if left unfulfilled
6.
INTOXICATION
It is aphysical or mental state
of exhilaration and emotional frenzy or
lathargy and stupor
WITHDRAWAL
It is the physiological and
mental readjustment that accompanies
the discontinuation of an addictive
substance
ALCOHOL
• Alcohol isa natural substance
formed by the reaction of fermentic
sugar with yeast spore
• It is a colourless
limpid,volatile,flamable,water misible
liquid
• Most states consider that an
individual is legally intoxicated with
the blood alcohol level of 0.08 to
0.10%
• Alcoholism is the inability to control
drinking due to both the physical and
emotional dependence on alcohol.
Biological factor:
i. Geneticvulnerability(family history of substance use
disorder: for example in type 2 alcoholism)
ii. Co-morbid psychiatric disorder or personality
disorder
iii. Co-morbid medical disorders
iv. Reinforcing effects of drugs (explains continuation of
drug use)
v. Withdrawal effects and craving(explains continuation
of drug use)
vi. Biomechanical factors for example, role of dopamine
and norepinephrine in cocaine, ethanol and opioid
dependence)
11.
Psychological Factor:
i. Curiosity:Need for novelty seeking
ii. General rebelliousness and social non-conformity
iii. Early initiation of alcohol and tobacco
iv. Poor impulse control
v. Sensation –seeking(high)
vi. Low self-esteem(anomie)
vii. Concern regarding personal autonomy
viii. Poor stress management skills
ix. Childhood trauma or loss
x. Relief from fatigue and/or boredom
xi. Escape from reality
xii. Lack of interest in conventional goals
xiii. Psychological distress
12.
Social Factor:
i. Peerpressure( often more important than parental
factors)
ii. Modelling (imitating behaviour of important others)
iii. Ease of availability of alcohol and drugs
iv. Strictness of drug law enforcement
v. Intra familial conflicts
vi. Religious reasons
vii. Poor social/familial support
viii. ‘Perceived distance’ within the family
ix. Permissive social attitudes
x. Rapid urbanisation.
13.
SIGNS AND SYMPTOMS
•Aggression
• Agitation
• Compulsive behavior
• Self distructive behavior
• Lack of restrained
• Black out
• Dizziness
• Shakkiness
• Craving
• Sweating
• Anxiety
• Euphoria
CLASSIFICATION
• According toJellinek
• Alpha
• Excessive and inappropriate drinking to relieve physical and
emotional pain
• No loss of control
• Beta
• Excessive and inappropriate drinking
• Due to cultural drinking pattern and poor nutrition
• No dependence
• Gamma
• Also called as malignant alcoholism
• Progressive course
• Physical dependence and psychological dependence
16.
Contd.,
• Delta
• Theamount of alcohol consumption
can be controlled
• Social disruption is minimal
• Epsilon
• Spree drinking
• Dipsomania (Compulsive drinking)
17.
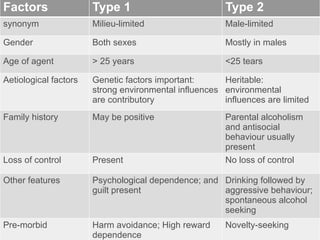
Factors Type 1Type 2
synonym Milieu-limited Male-limited
Gender Both sexes Mostly in males
Age of agent > 25 years <25 tears
Aetiological factors Genetic factors important:
strong environmental influences
are contributory
Heritable:
environmental
influences are limited
Family history May be positive Parental alcoholism
and antisocial
behaviour usually
present
Loss of control Present No loss of control
Other features Psychological dependence; and
guilt present
Drinking followed by
aggressive behaviour;
spontaneous alcohol
seeking
Pre-morbid Harm avoidance; High reward
dependence
Novelty-seeking
18.
PHASES OF ALCOHOLISM
•The pre alcoholic phase
• The early alcoholic phase
• The crucial phase
• The chronic phase
19.
• Prealcoholic phasecharacterised by the use of
alcohol to relieve the everyday stress abd tensions of
life
• Early alcoholic phase begins with blackouts- brief
periods of amnesia that occur during or immediately
following a period of drinking.
• In the crucial phase , the Individual has not control,
and physiological dependence is clearly evident.
• The chronic phase is characterised by emotional and
physical disintegration.
21.
Alcohol withdrawal
• Substancewithdrawal is the
development of a substance-specific
maladaptive behavioural
chamge,with physiological and
cognitive concomitants,that is due to
the cessation of, or reduction in ,
heavy and prolonged substance use
(APA ,2000). Withdrawal is usually,
but not always,, associated with
substance dependence.
22.
Alcohol withdrawal symptoms
•Anxiety
• Shaky hands
• Headache
• Nausea, vomiting
• Malaise or weakness
• Insomnia
• Sweating
• Hallucination
• Seizure
• Confusion
• Racing heart, Trachycardia
• Depressed mood or irritability
• Elevated BP
23.
Complications:
I. Medical Complications
A.Gastrointestinal System
i. Fatty liver, cirrhosis of liver, hepatitis, liver cell
carcinoma, and liver failure
ii. Gastritis, reflux oesophagitis, oesophageal varices,
Mallory-Weiss syndrome, achlorhydria, peptic
ulcer, carcinoma stomach and oesophagus
iii. Malabsorption syndrome, protein-losing enteropathy
iv. Pancreatitis: acute, chronic, and relapsing
24.
B. Central NervousSystem
i. Peripheral neuropathy
ii. Delirium tremens
iii. Rum fits (Alcohol withdrawal seizures)
iv. Alcoholic hallucinosis
v. Alcoholic jealousy
vi. Wernicke-Korsakoff psychosis
vii. Marchiafava-Bignami disease
viii. Alcoholic dementia
ix. Suicide
x. Cerebellar degeneration
xi. Central pontine myelinosis
xii. Head injury and fractures.
25.
C. Miscellaneous
i. Acnerosacea, palmar erythema, rhinophyma,
spider naevi, ascitis, parotid enlargement
ii. Foetal alcohol syndrome (craniofacial ano malies,
growth retardation, major organ system malformations)
iii. Alcoholic hypoglycaemia and ketoacidosis
iv. Cardiomyopathy, cardiac beri-beri
v. Alcoholic myopathy
vi. Anaemia, thrombocytopenia, Vitamin K factor
deficiency, haemolytic anaemia
26.
vii. Accidental hypothermia
viii.Pseudo-Cushing’s syndrome, hypogonadism,
gynaecomastia (in men), amenorrhoea, infertility,
decreased testosterone and increased LH levels.
ix. Risk for coronary artery disease
x. Malnutrition, pellagra
xi. Decreased immune function and proneness to
infections such as tuberculosis
xii. Sexual dysfunction
27.
II. Social Complications
i.Accidents
ii. Marital disharmony
iii. Divorce
iv. Occupational problems, with loss of productive man-
hours
v. Increased incidence of drug dependence
vi. Criminality
vii. Financial difficulties.
28.
DIAGNOSIS
• Spirometer
• BloodTest
• Urine Test
• Serum Electrolyte Analysis
• Liver function test
QUESTIONNAIRE
• Alcohol Use Disorders Identification Test
(AUDIT)
• Severity of Alcohol Dependence
Questionnaire ( SADQ)
• Alcohol Problem Questionnaire (APQ)
29.
Cage Questionnaire:
• TheCAGE questionnaire basically consists of four
• questions:
• i. Have you ever had to Cut down on alcohol
(amount)?
• ii. Have you ever been Annoyed by people’s criticism
• of alcoholism?
• iii. Have you ever felt Guilty about drinking?
• iv. Have you ever needed an Eye opener drink (early
• morning drink)?
• A score of 2 or more identifi es problem drinkers.
OT ASSESSMENT TOOL
•Occupational Self Assessment (OSA)
• Rosenberg Self-esteem Inventory
• Self Efficiency Scale
• Volitional questionnaire
• Coping Response Inventory
• Interest Checklist
• Role Checklist
• Assessment of Motor And Process Skills (AMPS)
• Internal /External Locus of Control Scale
• Occupational Performance History Interview (ll)
32.
• Alcohol andDrug Consequences Questionnaire (ADCQ)
• Alcohol Dependence Scale
• Barth Time Construction (BTC)
• Beck Depression Inventory (BDI-II)
• Brief Situational Confidence Questionnaire (BSCQ)
• Clinical Institute Withdrawal Assessment for Alcohol–Revised (CIWAA-R)
• Coping Behaviours Inventory (CBI)
• Drinker Inventory of Consequences (DRINC)
• Drinking Expectancy Questionnaire (DEQ)
• Form 90
• Inventory of Drinking Situations (IDS)
• Routine Task Inventory (RTI-2)
• Short Alcohol Dependence Data questionnaire (SADD)
33.
OT INTERVENTION
1. Cognitivebehaviour therapy
• Rational analysis
• Time projection
• Double stand dispute
• Thought stopping
• Bibliography
• Role play
• Re-labelling of thoughts
34.
• Behaviour Therapy
•Aversion therapy - using either a sub-threshold
electric shock or an emetic such as
apomorphine.
• Currently, in most settings, it is considered
unethical to use aversion therapy for the
treatment of alcohol dependence.
• covert sensitisation,
• relaxation techniques,
• assertiveness training,
• self-control skills
35.
• Psychotherapy
• Bothgroup and
individual psychotherapy have been
used. The patient should be
educated about the risks of
continuing alcohol use, asked to
resume personal responsibility for
change and be given a choice of
options for change. Motivational
enhancement therapy with or
without cognitive behaviour therapy
and lifestyle modification is often
useful, if available.
36.
Group therapy
• Oneof the important voluntary self-help
group is known as Alcohol Anonymous.
• It is the major self help organisation for
the treatment of alcoholism
• It was founded in 1935 by two Alcoholics
- Bill Wilson and Bob Smith
• The only Requirement of membership is
a desire on the part of the alcoholic
person to stop drinking
• There are 12 step that embody the
philosophy of AA
40.
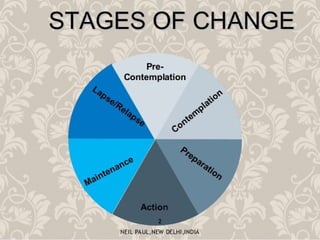
PRECONTEMPLATION
• People's arein this stage are not even
considering changing their drinking or using
behaviour
• They may be denial of their issues
• There are 4 reason for someone might be in
this stage
1. Reluctance
2. Rebellion
3. Resignation
4. Rationalisation
41.
CONTEMPLATION
• In thisstage where a person comes
to the realisation that they have a
problem
• They might want to change but not
feel like to do it
• At this stage people are researching
about the addiction and treatment
42.
DETEMINATION
• This isthe stage where the change
actually begins
• They will think about pros and cons
and make a decision to change
• They will decide to stop the drinking
and think about the future
43.
ACTION
• This isthe stage where the plans get
into a action
• They may start to attend AA meeting
or counselling
• This stage lasts approximately 3 - 6
months
44.
MAINTANANCE AND RELAPSE
•In this stage people become adapted to an
alcohol free life
• Relapse - Reestablish the previous pattern. Initial
return to use
• The risk of Relapse will be present because
substance use disorder is a chronic condition
TERMINATION
• According to DiClemente and prokasha the
ultimate goal of the stages of addiction recovery
and change is termination
• This is the stage where the person no longer
feels, threatened by their drugs or drink of choice
45.
RELAPSE PREVEVENTION
GENERAL PRINCIPLE
•Self regulation and stabilisation
• Integration and self assessment
• Understanding and Relapse
education
• Self knowledge and identification of
warning signs
• Coping skills
• Change and recovery planning
• Awareness
• Significant involvement of others
46.
INTERVENTION
• Support ofthe family and friends
• 12 step meeting
• Individual and group therapy
• Family therapy
• Proper rest
• Moderate exercise and nutrition
• Avoidance of slippery situation such
as bars
• Medical supervision
• Psychiatric support