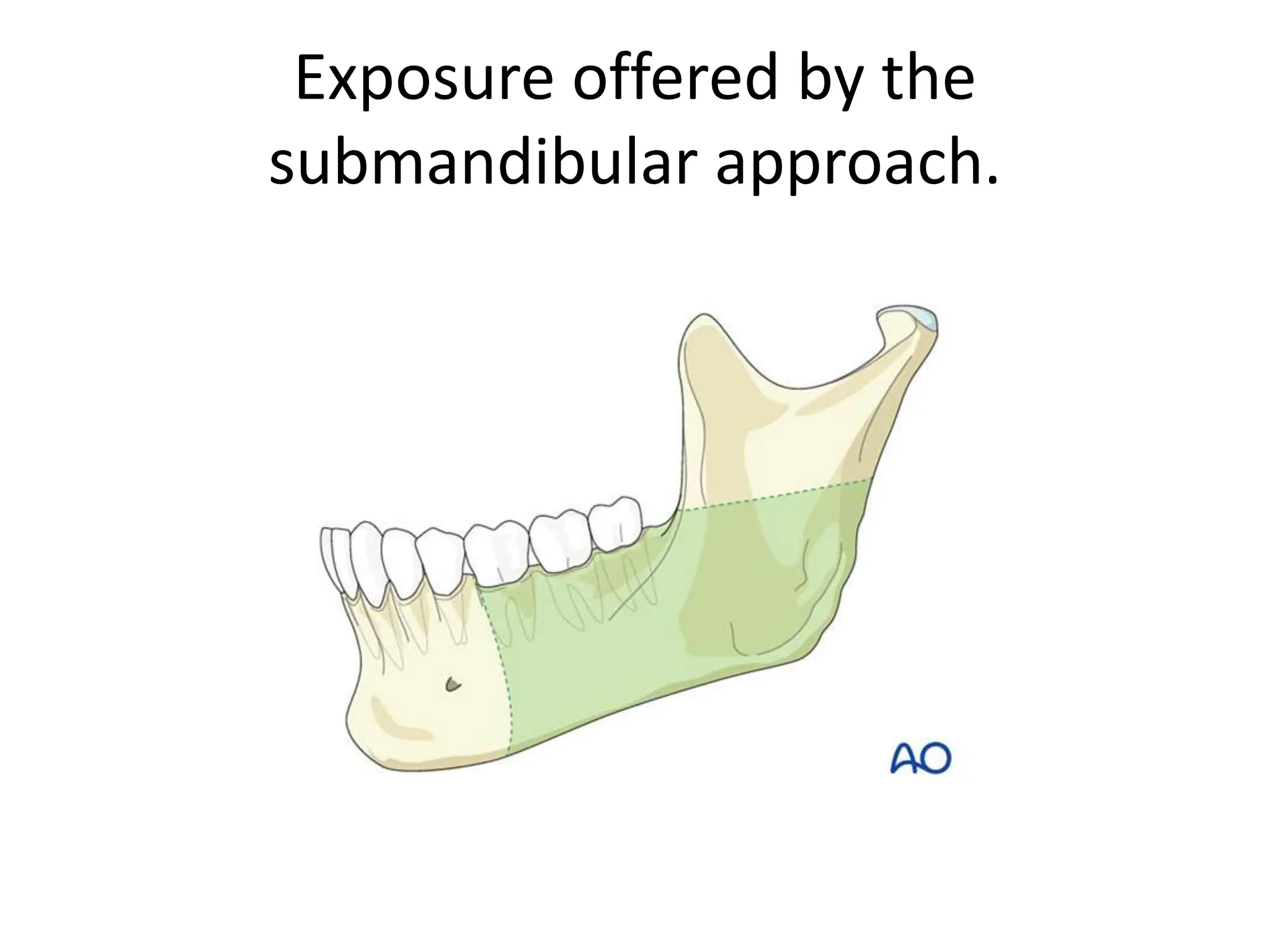
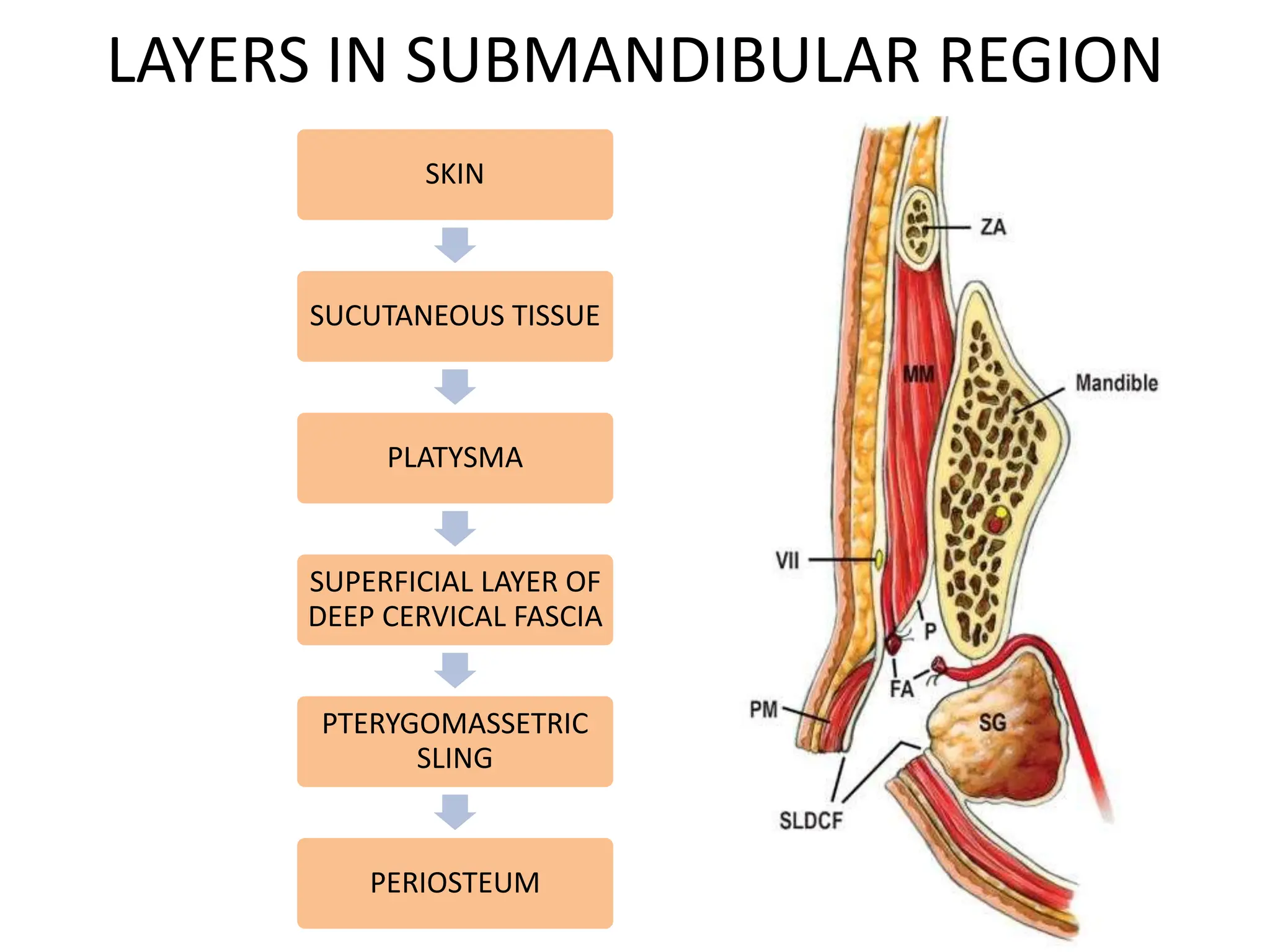
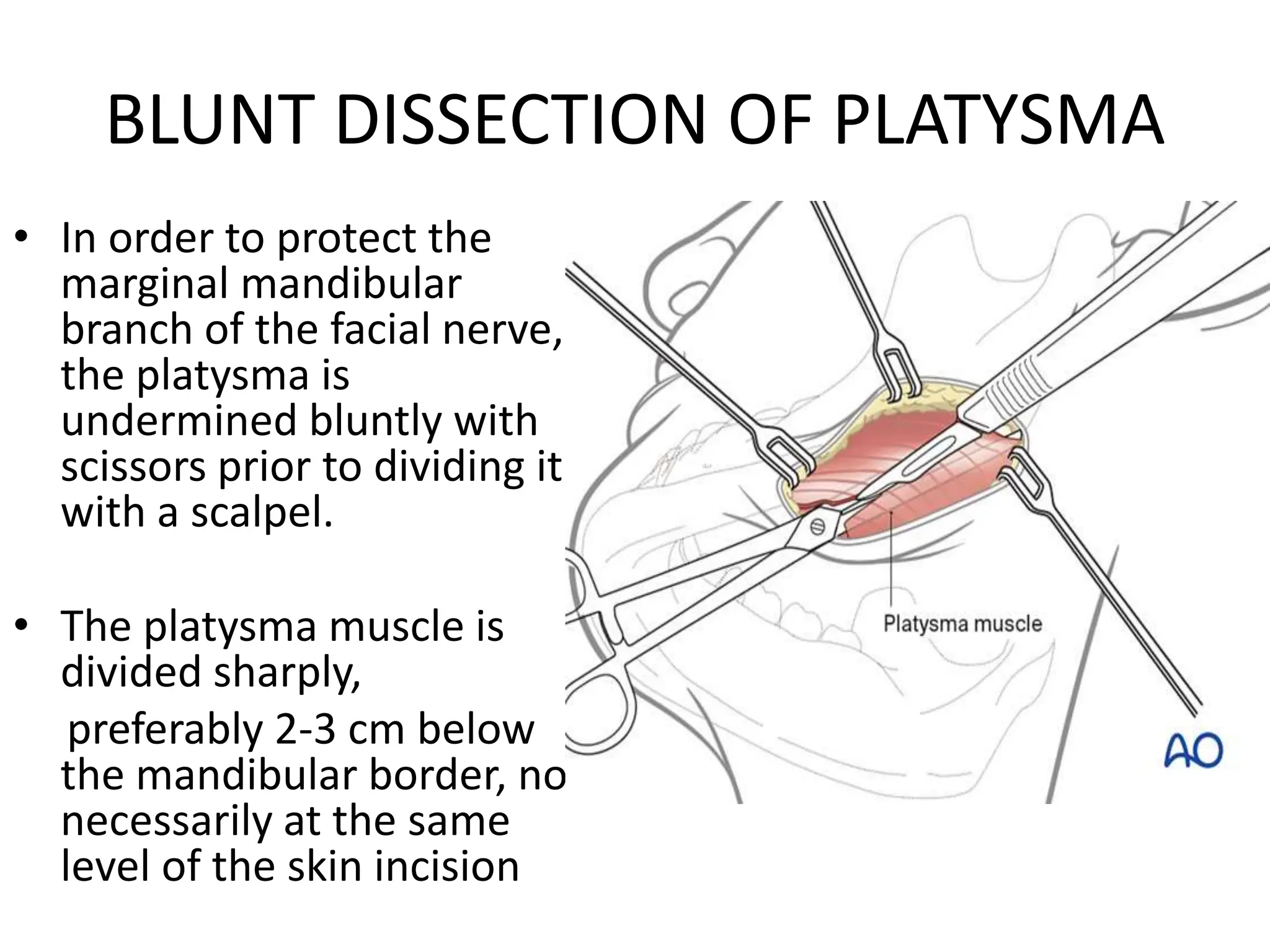
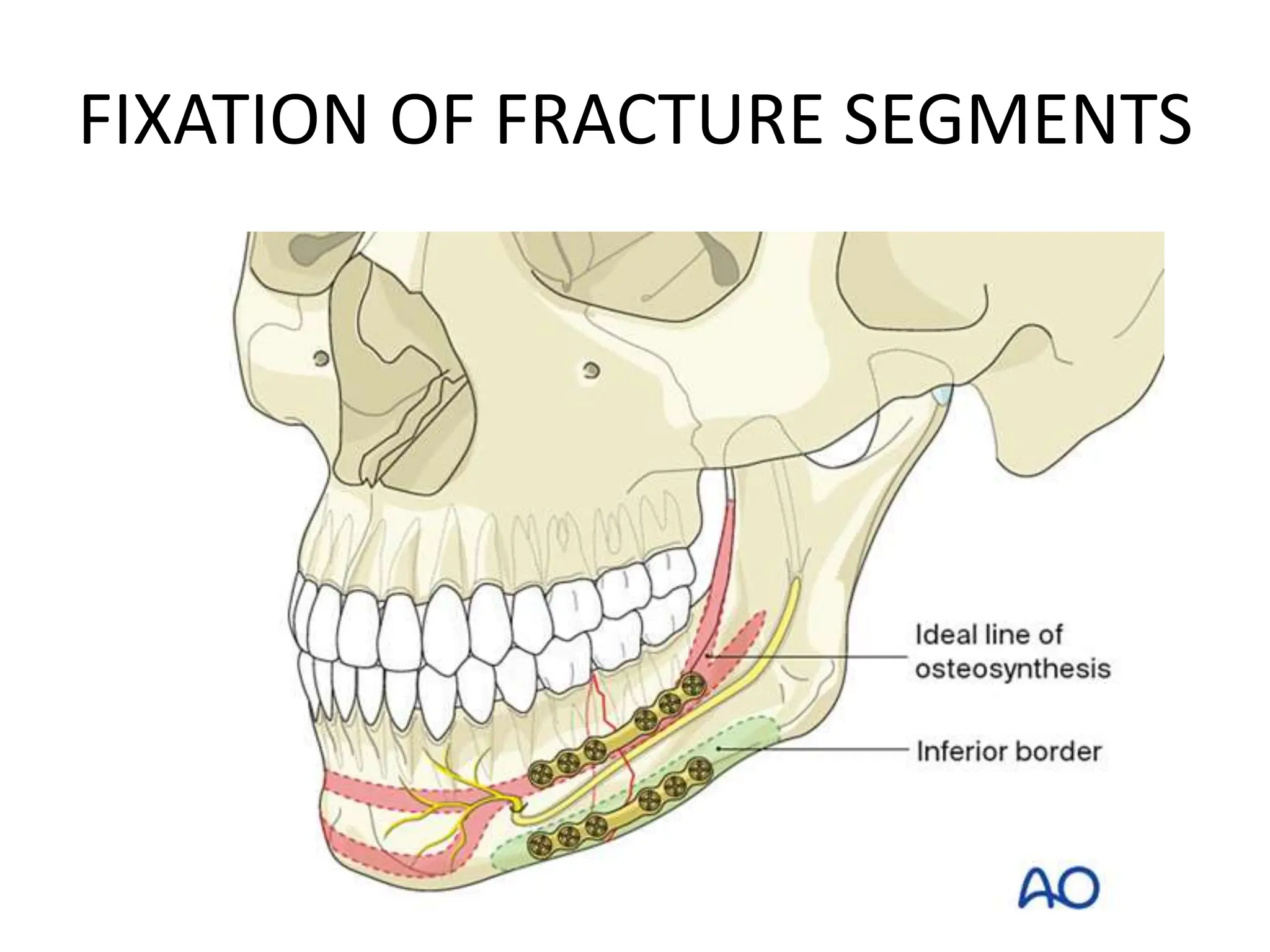
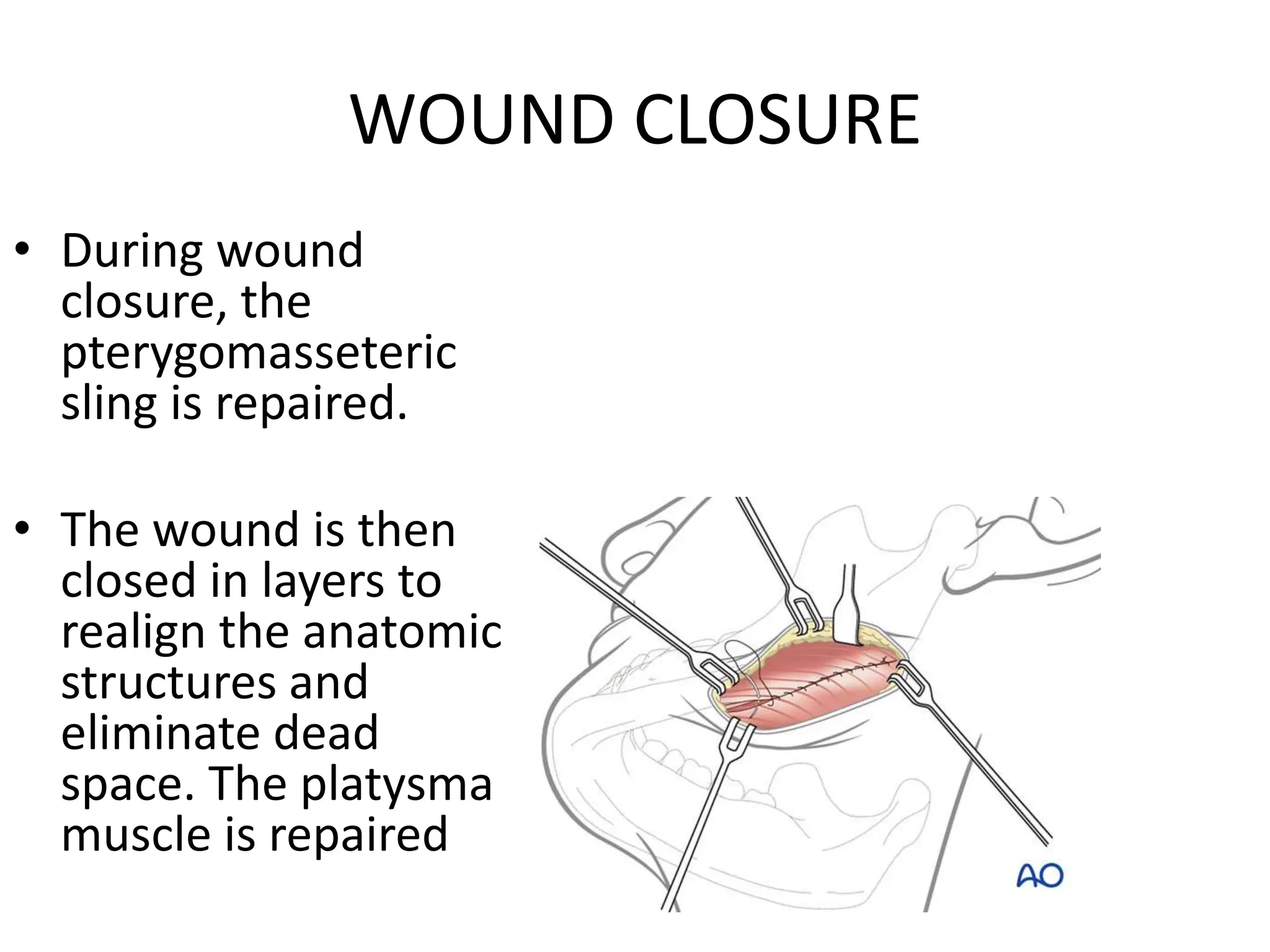
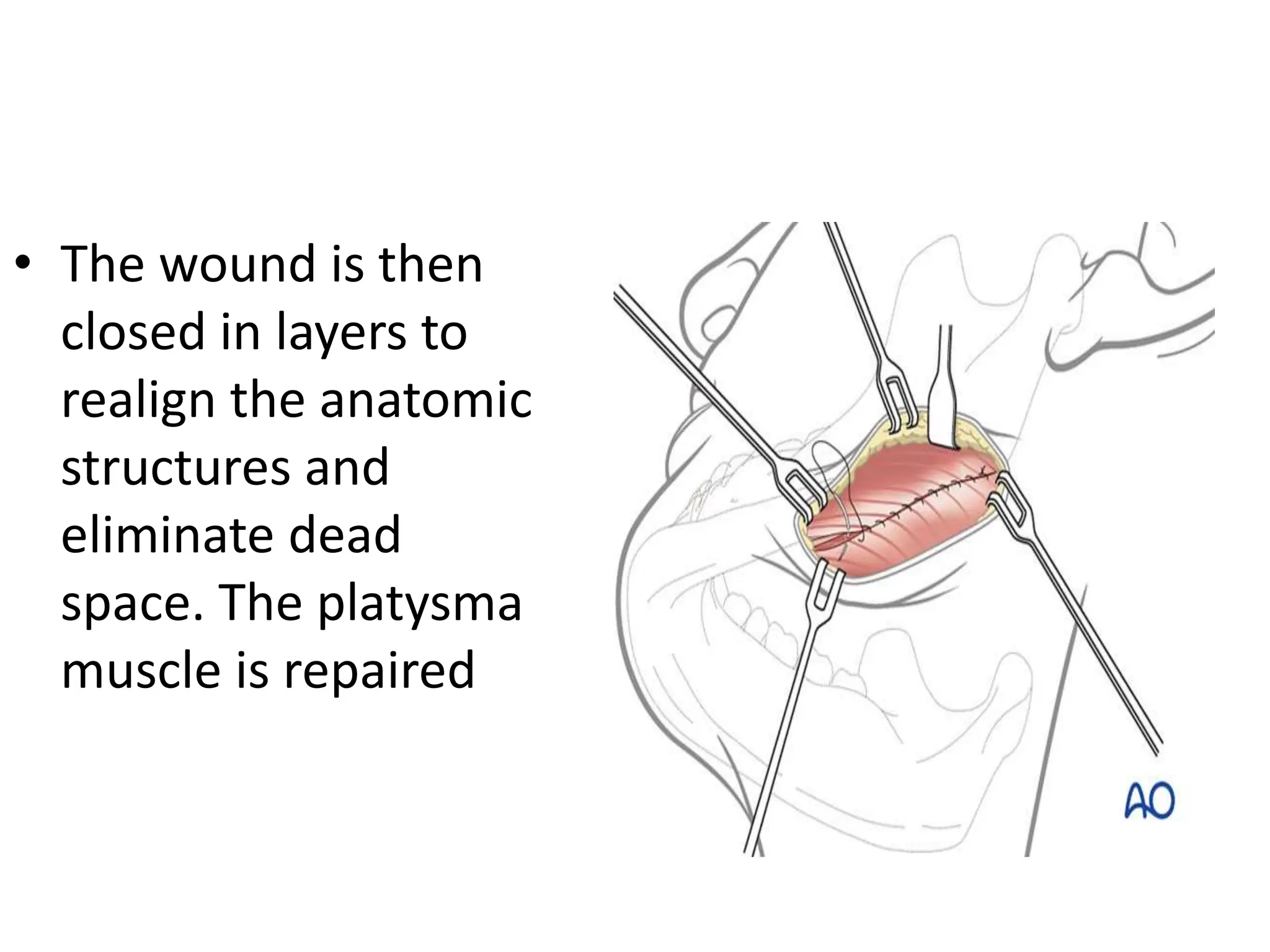
The submandibular approach by Dr. Ashish is indicated for challenging mandibular body and angle fractures unsuitable for intraoral treatment. The technique involves specific skin incisions, careful dissection to protect vital structures, and layered wound closure to ensure anatomical realignment. Proper exposure and fixation of fracture segments are critical for successful outcomes in these complex cases.