Download to read offline

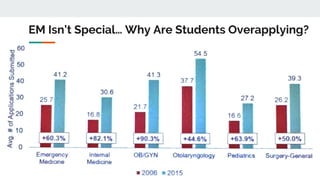


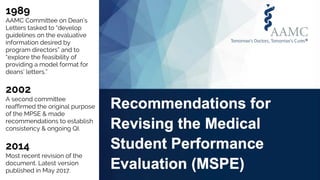
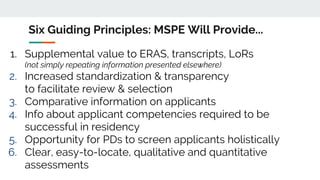




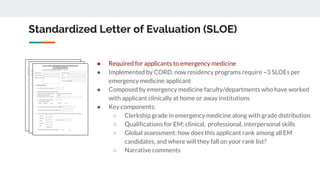
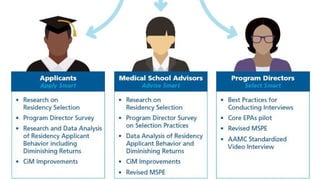

The document discusses strategies for streamlining the residency application and match process, with a focus on innovations in applicant screening and selection in emergency medicine. It highlights the need for better tools to address issues of overapplication and introduces the standardized video interview to evaluate non-academic competencies of applicants. Recommendations for revising the Medical Student Performance Evaluation are also provided to enhance its effectiveness in assessing students holistically.


















































































