Hypoxic ischemic insult, by prof Ayman Galhom, ass prof neurosurgery, Suez ca...mohamed osama hussein
A lecture given by dr Ayman Galhom, assistant professor neurosurgery, Suez canal university, during Port said fourth neonatology conference, at 24-25 October, 2013. This lecture was a discussion of the pathophysiology & management of hypoxic ischaemic insult to an infant in PICU
Hypoxic ischemic insult, by prof Ayman Galhom, ass prof neurosurgery, Suez ca...mohamed osama hussein
A lecture given by dr Ayman Galhom, assistant professor neurosurgery, Suez canal university, during Port said fourth neonatology conference, at 24-25 October, 2013. This lecture was a discussion of the pathophysiology & management of hypoxic ischaemic insult to an infant in PICU
Pathophysiology of TBI is complex and consists of acute and delayed injury. In the acute phase, brain tissue destroyed upon impact includes neurons, glia, and endothelial cells, the latter of which makes up the blood-brain barrier. In the delayed phase, “toxins” released from damaged cells set off cascades in neighboring cells eventually leading to exacerbation of primary injury. As researches further explore pathophysiology and molecular mechanisms underlying this debilitating condition, numerous potential therapeutic strategies, especially those involving stem cells, are emerging to improve recovery and possibly reverse damage. In addition to elucidating the most recent advances in the understanding of TBI pathophysiology, this review explores two primary pathways currently under investigation and are thought to yield the most viable therapeutic approach for treatment of TBI: manipulation of endogenous neural cell response and administration of exogenous stem cell therapy.
The most common cause of death in young is non other than Head injury. The modern advances not only gave human mankind a luxury but with high velocity injury there is high burden of head injury too. This slide is updated with BTF 2016 guideline
Alzheimer's disease is a progressive disorder that causes brain cells to waste away (degenerate) and die. Alzheimer's disease is the most common cause of dementia — a continuous decline in thinking, behavioral and social skills that disrupts a person's ability to function independently.
Symptoms: Amnesia; Dementia
Diseases or conditions caused: Dementia
Pathophysiology
Pathology
BPharm 2nd Semester
MPharm
Therapeutics
MBBS
A feature about latest research to improve premature babies' medical care.
Published in The Lancet Neurology:
http://www.lancet.com/journals/laneur/article/PIIS1474-4422%2813%2970041-3/fulltext
A presentation about Alzheimer's disease, it's definition, it's etiology, its mechanism of development as well as actual treatment and developing treatments.
1. Stem cell therapies for perinatal brain injuries
Reaz Vawda a
, Jennifer Woodbury a
, Matthew Covey a
,
Steven W. Levison, Huseyin Mehmet*
RY80Y-215, Merck Research Laboratories, 126E Lincoln Avenue, Rahway, NJ 07065, USA
KEYWORDS
Children;
Head injury;
Hypoxia;
Ischaemia;
Regenerative medicine;
Stem cells
Summary This chapter reviews four groups of paediatric brain injury. The pathophysiology of
these injuries is discussed to establish which cells are damaged and therefore which cells rep-
resent targets for cell replacement. Next, we review potential sources of cellular replace-
ments, including embryonic stem cells, fetal and neonatal neural stem cells and a variety of
mesenchymal stem cells. The advantages and disadvantages of each source are discussed.
We review published studies to illustrate where stem cell therapies have been evaluated for
therapeutic gain and discuss the hurdles that will need to be overcome to achieve therapeutic
benefit. Overall, we conclude that children with paediatric brain injuries or inherited genetic
disorders that affect the brain are worthy candidates for stem cell therapeutics.
ª 2007 Published by Elsevier Ltd.
Clinical considerations
Perinatal hypoxic/ischaemic brain injuries
Hypoxiaeischaemia (H/I), which refers to both lack of
blood flow and low oxygen tension in the brain, is
associated with neurological deficits that range from severe
cerebral palsy to mild developmental disabilities.1
The
causes of H/I are complex and heterogeneous, including
stress during labour, cardiac insufficiency of the mother,
placental damage, prolapsed umbilical cord, uterine rup-
ture and acute neonatal or maternal haemorrhage. The
outcome from H/I is further influenced by a variety of fac-
tors that include the age of gestation, length of H/I, type of
insult and external factors. External factors include mater-
nal as well as fetal factors, such as cardiopulmonary insuf-
ficiency and immune status.
Term and preterm infants sustain different types of
injury. The type and severity of brain damage sustained by
the term infant is modulated by infection, extended labour
or repeated asphyxia after birth. Five general classes of
pathology are observed after H/I insults in the term infant:
selective neuronal necrosis, status marmoratus, parasagit-
tal cerebral injury and focal and multifocal ischaemic brain
necrosis.2
These injuries are caused by pathophysiological
events that are not fully understood. What is clear is that
transient energy failure sets off a chain of events leading
to cerebral cell death. With energy depletion, ionic homeo-
stasis fails, causing disturbances in Naþ
, Kþ
and ClÀ
.3,4
Neu-
rons depolarize, releasing excitatory amino acids (EAAs),
resulting in excitotoxicity.5
EAAs open neuronal N-methyl-
D-aspartate (NMDA) receptors, resulting in high levels of
free Ca2þ
as well as increases in water and other cations.6,7
Elevated intracellular calcium, in turn activates proteases,
* Corresponding author. Tel.: þ1 732 594 2511; fax: þ1 732 594
8255.
E-mail address: huseyin_mehmet@merck.com (H. Mehmet).
a
These authors contributed equally.
1744-165X/$ - see front matter ª 2007 Published by Elsevier Ltd.
doi:10.1016/j.siny.2007.02.003
available at www.sciencedirect.com
journal homepage: www.elsevier.com/locate/siny
Seminars in Fetal & Neonatal Medicine (2007) 12, 259e272
2. endonucleases, phospholipases, caspases and calpains,
leading to cell death.8e15
EAAs also activate AMPA/kainate
receptor/channels, causing oligodendrocyte progenitor cell
death.16
Reperfusion after H/I also triggers the production
of oxygen free radicals.4,17
During an H/I insult, the natural
defences of the cells are overwhelmed, leaving them vul-
nerable to free-radical-mediated damage. Cell death also
induces an inflammatory response,18
which can e directly
or indirectly e lead to secondary cell death.19,20
The damage sustained by the preterm infant has been
classically referred to as periventricular leukomalacia
(PVL), which is defined as focal and diffuse damage to the
periventricular white matter. With advances in the clinical
management of low birth weight infants, focal lesions of
the white matter are less commonly seen, although
abnormalities in the subcortical white-matter damage
appear in 75% of preterm infants on magnetic resonance
imaging (MRI).21,22
More recently, it is beginning to be ap-
preciated that very low birth weight and low birth weight
infants have a reduced cortical grey matter volume at
term equivalent that is still present at 8 years of age.23e25
When these scans are correlated with neurodevelopmental
outcomes measured at 18e20 months corrected age they
are highly predictive of adverse outcome.26
Studies on ani-
mal models suggest that this reduced volume of cortical
grey matter is due to neuronal cell death, where subplate
neurons are especially vulnerable, thereby affecting the
formation of appropriate connections from subcortical re-
gions of the brain. Oligodendrocyte progenitors both in
grey and white matter are vulnerable and changes in synap-
togenesis have been documented.27e31
The pathophysiology observed in the preterm infant is
not identical to the term infant because of developmental
and maturation differences. The cerebrovascular system of
the premature infant is underdeveloped, resulting in both
incomplete local and global cerebral blood.32
In addition,
the immature vessels have poor cerebrovascular autoregu-
lation.33
The subcortical white matter of the premature in-
fant is especially poorly vascularized, which predisposes
this region to damage. In addition, oligodendrocyte progen-
itors are extremely vulnerable to damage during an H/I in-
sult.34
Specifically, oligodendrocyte progenitors at the O4þ
stage are highly sensitive to glutamate toxicity and lack the
ability to detoxify free radicals.35e37
(Fig. 1)
Paediatric traumatic brain injuries
Children who have sustained traumatic brain injuries
represent another group of patients who might benefit
from stem cell therapies. Traumatic brain injury (TBI) is
a major cause of death in the paediatric age group, and
approximately 475,000 children under the age of 14 sustain
a TBI yearly, and estimates are that 30,000e100,000
children aged <1 year sustain a TBI that requires admitting
them to an intensive care unit yearly.38
Although the most
common cause of injury is a motor vehicle accident, the
many other causes of paediatric brain injury include as-
sault, in the form of shaking as a form of punishment, which
is a major cause of TBI in infants.38
The extent of damage to
the perinatal brain depends on several factors, including
the size and object causing the injury, location of injury,
force of impact, and whether it is penetrating or blunt
and open or closed. It is important to recognize that exter-
nal signs might not indicate the severity of the injury.
Whereas skull fractures and lacerations might not damage
the brain parenchyma, a closed injury can cause quite se-
vere destruction.
Blunt head injury can cause: (1) focal haemorrhagic and
non-haemorrhagic lesions mainly involving grey matter; (2)
diffuse axonal injury (DAI); and (3) secondary injury caused
by oedema and space-occupying haemorrhages.39
Analogous
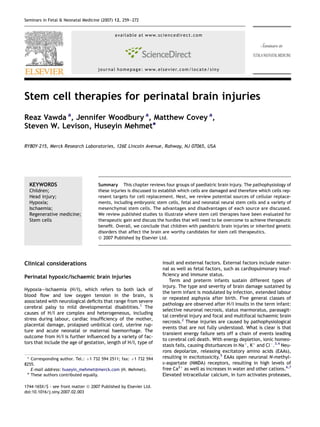
Figure 1 Severe hypoxic ischaemic encephalopathy. Severe hypoxiceischaemic encephalopathy in newborn infants leads to loss
of grey and white matter, with subsequent neurodisability. T1 transverse MR images of two infants with severe brain injury follow-
ing hypoxiceischaemic encephalopathy. (a) Transverse image acquired in an infant at 18 days of age demonstrating large areas of
low signal intensity in the white matter (arrows), which later atrophy. (b) An image at the level of the basal ganglia of an infant at
20 days of age showing loss of grey and white matter with cystic change in the basal ganglia (arrow).
260 R. Vawda et al.
3. to H/I injury, oxidative stress, excitotoxicity and mitochon-
drial dysfunction are major effectors of cell death, with
neuroinflammation, diffuse brain swelling and vascular al-
terations also contributors to the net outcome.40,41
Rodent models of TBI indicate that after lateral fluid
percussion brain injury, which models the type of injury
sustained as a result of head trauma during a motor vehicle
accident, there is both focal and diffuse brain injury.42
DAI
is often observed distal to the site of focal injury where the
damage is more cell-type specific and where neurons are
more selectively damaged than glial cells.43,44
Concussive
injuries to the head often involve shearing forces that cause
DAI in the subcortical white matter. Subsequent to the ini-
tial injury, there is often secondary or delayed injury (pro-
gressing from hours to months following injury and likely to
be partially reversible). The mechanisms of secondary in-
jury are complex and poorly understood, but include the
breakdown of the bloodebrain barrier (BBB), oedema,
vasospasm, ionic dysregulation, lipolysis, EAA toxicity,
free-radical generation, impairment and/or uncoupling of
energy metabolism, changes in intracranial pressure (ICP)
and or cerebral perfusion pressure (CPP), inflammation,
expression of both pathogenic and protective genes and
proteins and activation and/or release of autodestructive
factors. Whereas the initial insult typically causes necrotic
cell death, the cells that die during the second wave of in-
jury typically die of apoptotic cell death.45e47
As the brain
attempts to cope with the extensive tissue damage that has
occurred there is a strong astrogliotic response. This is ben-
eficial in that the bloodebrain barrier is restored and there
is some restoration of structural integrity; however, a glial
scar is typically formed and this inhibits regeneration.
Thus, in contemplating how to repair the TBI brain, one
must take into consideration the fact that multiple cell
types are damaged, and that the cells that survive might
not entirely resemble their premorbid state. Surviving neu-
rons might no longer be connected to their targets as a con-
sequence of diffuse axonal injury, there might be selective
elimination of specific neuronal cell types as a result of dif-
fuse damage, and the glial cells that once nourished their
neighbours might now be components of an anisomorphic
gliotic scar.
Like H/I, the severity of the TBI insult depends on many
different factors, including the age and state of the infant,
as well as the duration and type of injury. The injury can
manifest differently depending on the location of the
injury, and range from physical disabilities to memory
problems to social, emotional or behavioural difficulties.
The developing infant up to 4 years of age does respond dif-
ferently to TBI than an older child with a similar insult.48
Using MRI technology, Tasker has shown that there is
white-matter damage, especially in the hippocampus, in
adults who sustained TBI as a child, and thus it will be
safe to assume that these types of injuries will result in
long-term consequences.39
Metabolic diseases
A handful of metabolic diseases might benefit from stem cell
therapies in the perinatal brain. The scope of metabolic
syndromes extends from lysosomal, peroxisomal, mitochon-
drial and amino acid disorders to neurodegenerative
diseases and muscle diseases. The majority of such disor-
ders are seen in early childhood with progressive neurolog-
ical deterioration, while some manifest severely at birth.
Neuronal death results from the accumulation of substrates
in the cells due to a deficiency of an enzyme specific to the
catabolism of sphingolipids, mucopolysaccharides or muco-
lipids. Leukodystrophies include some lysosomal and perox-
isomal diseases that involve problems with the myelination.
Most metabolic syndromes are genetic in nature; autosomal
recessive inheritance is the most common but other forms
include autosomal dominant, mitochondrial and X-linked
disorders. Although it might not be necessary to determine
the genetic nature of the disease, the specific cellular
pathology is important to better understand which cell
population is most affected and what stem cell therapy
would be able to offer.
Peroxisomal disorders can be divided into two broad
categories depending on whether there is a problem with
peroxisome biogenesis or a single enzyme deficiency.
Zellweger’s syndrome is a severe form of a disorder caused
by a deficiency in peroxisomal biogenesis; adrenoleukodys-
trophy is a less severe form. Zellweger’s syndrome e also
known as cerebrohepatorenal syndrome e is a rare, auto-
somal recessive metabolic disease and is the most severe
phenotype of this group. It is characterized by severe
nervous system dysfunction, craniofacial abnormalities
and hepatic fibrosis. There is a build up of cerebral neutral
lipids and very long-chain fatty acids because peroxisomes
are unable to oxidize these and mitochondria are over-
whelmed. In the most severe cases, infants rarely live past
1 year. All Zellweger’s patients have defective peroxisome-
targeting sequences, PTS1 and PTS2 proteins, and 80% have
mutations in PEX1 and PEX6, which encode the ATPases re-
quired for peroxisome membrane biogenesis. Other muta-
tions have also been shown to decrease the number of
functional peroxisomes, such as PEX13. Interestingly, there
is a clear correlation between the number of peroxisomes
and the degree of severity of the disease. Pathological
studies have shown maldevelopment, especially in the
CNS, including neuronal migration abnormalities, cerebel-
lar atrophy and white-matter disease.49
Adrenoleukodystrophies are a less severe phenotype
than Zellweger’s syndrome but also include a defective
peroxisomal transporter. Although there is an X-linked form
of the disease, only the autosomal disorder with neonatal
onset will be discussed here. Affected children suffer from
hypotonia and seizures due to an inability to oxidize very
long-chain fatty acids, this inability results in lipid accu-
mulation. The disease is characterized by progressive de-
generation of the CNS white matter and adrenal gland.50
Additionally, the typical symmetrical, inflammatory, demy-
elinating lesions of this disease involve the cerebral and
cerebellar white matter, with both axonal loss and a de-
crease in oligodendrocytes.51
Lysosomal storage diseases are another potential stem-
cell therapy recipient. When grouped together, the in-
cidence rate is estimated 1 in 18,000 live births, and they
are considered a major cause of paediatric neurodegener-
ative disease.52,53
As in the peroxisomal disorders, we will
emphasize the neonatal forms, appreciating that these
disorders exist in juvenile and adult forms as well. As
expected, the infantile forms are most severe, usually
Stem cells for brain injuries 261
4. involving acute brain damage, and patients rarely live past
a few years of age. CNS symptoms, such as seizures, de-
mentia and brainstem dysfunction can complement periph-
eral symptoms, such as hepatosplenomegaly, heart and
kidney injury, muscle atrophy and abnormal bone forma-
tion, but they vary in the different phenotypic profiles of
individual diseases.52,53
Some diseases show more neurolog-
ical signs than peripheral symptoms in the neonatal form,
such as TayeSachs and type 2 Gaucher disease, which
show severe neurological impairment. TayeSachs disease
is a hereditary ganglioside storage disease due to a defi-
ciency in the hydrolytic enzyme, b-hexoaminidase; type 2
Gaucher disease is a glucocerebrosidase deficiency that re-
sults in a glucocerebroside storage disorder. The build-up of
these materials, whatever the substrate, is detrimental to
the neurons of the CNS.52,53
White-matter diseases
The common pathology of white-matter diseases is myelin
deficiency, either in the form of hypo- or dysmyelination
during development or demyelination in the postnatal
brain.54
The oligodendrocyte is clearly affected in these dis-
eases, however, it is becoming clear that their demise might
be secondary to dysfunction of white matter astrocytes.
Some of these leukodystrophies are caused by genetic muta-
tions in oligodendrocytes whereas others are a consequence
of astrocytic genetic mutations.54,55
Vanishing white-matter
(VWM) disease is a childhood disease that has an infantile
variant called Crees leucoencephalopathy. It is character-
ized as central demyelination, with progressive neurode-
generation, cerebellar ataxia, and sometimes seizures and
optic atrophy. It is caused by a mutation in any one of the
five subunits of eukaryotic translation initiation factor
eIF2B, which is important for protein synthesis. The severe
infantile variant affects infants between 3 and 9 months
with failure to thrive, irritability, feeding problems, limb hy-
potonia or hypertonia, seizures, coma and death by 2 years
of age. The prominent cell type affected in VWM disease is
the oligodendrocyte, showing an overall loss with an appar-
ently high number of mature oligodendrocytes, as well as
dysmorphic, astrocytes with blunt processes.56
Canavan disease is interesting because it is caused by
a genetic mutation in the aspartoacylase (ASPA) gene,
which is a metabolic enzyme restricted to the CNS and e
more specifically e to oligodendrocytes.57
As in VWM dis-
ease, the congenital and infantile types are the most severe
forms of the disease, exhibiting widespread vacuolization in
the lower cerebral layers and white matter, with a lack of
myelin.57
Canavan disease is estimated at 1 in 5000 live
births in the Ashkenazi Jewish population. Interestingly,
there is astrocytic involvement in this disease, with the hy-
pothesis that vacuoles are generated from ruptured astro-
cytes that split the myelin lamellae, which then disperse
and widen to form extracellular sponginess.
Alexander disease is an autosomal dominant disorder
caused by a dominant gain-of-function mutation in the
GFAP gene, causing toxicity in a still unknown manner. In-
termediate filament inclusions, known as Rosenthal fibres,
accumulate within astrocytes, whereas oligodendrocytes
appear histologically normal. Symptoms of the infantile
form of include progressive psychomotor retardation, loss
of developmental milestones, megalencephaly, seizures,
ataxia, hyperreflexia, and pyramidal signs, with death usu-
ally ensuing by 2 years of age.58
(Fig. 2)
Sources of stem cells
From the outset it must be emphasized that there are many
different types of stem cell, which have a greater or lesser
utility for repairing the damaged brain. As a consequence
of this variety there can be no single definition for a stem
cell, although the following characteristics are shared by
most cells classified as stem cells. Stem cells are karyo-
typically normal, undifferentiated, possess extensive pro-
liferative capacity, are capable of long-term self-renewal
Figure 2 White-matter abnormality in extremely preterm infants. T2-weighted transverse MR images. (a) Image of a preterm
infant at term-corrected age demonstrating patchy high signal intensity in the white matter (arrows). Overt white-matter cystic
change (periventricular leukomalacia) is now very rare but more subtle white-matter signal change on MR imaging occurs in the
majority of infants at 28 weeks. This pattern represents abnormality59
and is not present in normal term-born infants. (b) This
MR feature probably represents loss or maldevelopment of oligodendrocytes and their precursors.
262 R. Vawda et al.
5. and are multipotent. Stem cells that are being considered
and evaluated for neural cell replacement include embry-
onic stem cells, embryonic germ cells, embryonic carinoma
cells, fetal and postnatal neural stem cells, bone marrow
stromal cells, placental stem cells and umbilical cord stem
cells (Fig. 3). For many cell replacement strategies, ex-vivo
expansion and specification will be required before
transplantation.
Embryonic stem cells
Embryonic stem (ES) cells are totipotent (i.e. they give rise
to all tissues in the body, including those of the nervous
system).60
As such, they are a promising starting material
for therapeutic applications. Undifferentiated ES cells ex-
press genes such as Oct-4, SSEA-1, SSEA-3, SSEA-4, TRA
1e60, TRA 1e81 and nanog.61
They can be propagated in vi-
tro and can be engineered to express therapeutic genes.
The first demonstration that mouse ES cells can be
differentiated into multiple neural phenotypes in culture
was reported by Bain and colleagues62
using retinoic acid.
The newly formed neurons not only expressed lineage-spe-
cific markers but were also capable of generating action po-
tentials. Several groups have now enriched neural
progenitors from murine and human ES cells.63,64
The latter
can incorporate into brain tissue and differentiate in vivo.65
ES cells provide the most promising source of cells for
therapeutic transfer into neural tissue. They are multi-
potent, can be propagated in vitro and can be engineered to
express therapeutic genes. They migrate and differentiate
into regionally appropriate cell types and do not appear to
interfere with normal brain development.66
ES cells can also
be differentiated in vitro into oligodendrocyte precursors
that effectively myelinate host axons in animal models of
human demyelinating disease.67,68
Early successes in neural differentiation of ES cell grafts
in vivo has led to further work in injury models to
demonstrate that transplanted ES cells can integrate and
functionally improve outcome following CNS injury.69,70
However, it is clear that there is still a significant gap in
our knowledge of how to direct the appropriate differenti-
ation of ES cells into specific lineages in vivo.
Ignoring the restrictions placed on using ES cells, the
capacity of ES cells for unlimited growth in culture reflects
their tendency to form teratomas after implantation. Until
reliable means of completely eliminating undifferentiated
ES cells from populations intended for implantation are
developed and tested, ES cells remain an experimental tool
with which to explore proof-of-principle therapies for
neurodegenerative conditions.
Neural stem cells: fetal and postnatal
Traditionally, the precursors of the CNS are classified as
either primary or secondary neuroepithelial cells. Primary
neuroepithelial cells are direct descendants of the neural
plate and reside in the walls of the ventricles as so-called
ventricular zone (VZ) cells. Like the cells of the primitive
neuroepithelium, the cells of the VZ extend processes that
span the width of the developing CNS. These cells form
a pseudostratified epithelium. As development proceeds,
progeny of the VZ become postimitotic neuroblasts. They
leave the VZ to migrate apically towards the pial surface
using radial glia as their guide.71,72
The progeny of the VZ
colonize specific cortical laminae as dictated by their birth
date, with earlier-born neurons generally settling into the
Figure 3 Sources and strategies using stem cells for neural cell replacement.
Stem cells for brain injuries 263
6. deeper laminae and later-born neurons migrating past them
to colonize more superficial layers.73
In this manner, the
layered cortices of the brain are formed in an inside-out
pattern. Beginning with the report by Gray and Sanes,74
it
has become clear that radial glia divide in a self-renewing
manner and are capable of producing both neurons and as-
trocytes; hence, they can no longer be regarded simply as
guides for emigrating neuroblasts but also as bipotential
neural stem cells (NSC).75e78
Another important realization
is that the radial glia of the VZ predominantly generate the
large projection or pyramidal neurons.
The emergence of the first neurons coincides with the
appearance of another proliferative population subjacent
to the VZ. These secondary neuroepithelial cells reside the
subventricular zones (SVZ). As the VZ decreases in promi-
nence the SVZs expand. They peak in humans in the
35th week of gestation,79
whereas in the rodent they
peak in number during the first postnatal week.80
The
SVZs are densely populated and SVZ cells can be identified
as far caudally as the third and fourth ventricles. At the
light microscopic level, SVZ cells are small, compact cells
that are usually round or oval and have little cytoplasm
and few organelles. SVZ cells often possess a single thin
process, and this process is not necessarily oriented per-
pendicular to the pial surface as are those of VZ and radial
glia cell processes.
The fetal brain contains large expansions in the ventral
forebrain. These expansions e termed the ganglionic
eminences e are an important source of the interneurons
of multiple subcortical nuclei, including the basal ganglia,
hippocampus and thalamus, they are also an important
source of the interneurons of the neocortex. As fetal
development proceeds the ganglionic eminences recede,
but a prominent SVZ persists at the dorsolateral angles of
the lateral ventricles. Studies on rodents have shown
that this region is a prominent source of GABAergic in-
terneurons that populate the olfactory bulb,81,82
as well as
a major source of macroglia, especially the myelinating
oligodendrocytes.83,84
The brain also contains another mitotically active area
that participates in development and is retained through-
out life, the subgranular zone (SGZ) of the hippocampus.
The SGZ is formed from a specialized pool of cells in the SVZ
at approximately the same period.85
As the number of pre-
cursors expands, these granular cells migrate radially to the
area where the primordial granular layer is formed. Once in
place, the cells proliferate locally and, by approximately
postnatal day (P) 10 in the rodent, an identifiable layer of
precursor cells is visible at the border between the granular
layer and the hilus of the hippocampus. From this region,
granule cells, which populate the hippocampus, are born
throughout life.
In-vivo and in-vitro studies have provided evidence of
cells distributed throughout the brain that continue to
divide throughout the life span. These cells are clearly
a source of additional glial cells and in-vitro studies have
shown that they can also behave as stem cells.86e88
How-
ever, whether these cells actually participate in generating
new neurons in vivo remains quite controversial.89,90
Although the bulk of experimental data has been obtained
using rodent NSCs, similar multipotent cells have been
identified in the human.91,92
When considering NSCs for replacement therapies, it is
important to recognize that cells from different gestational
ages and anatomical sites are not identical, displaying
different growth characteristics, trophic factor require-
ments and specific patterns of differentiation.93e97
Fetal NSCs can be propagated rapidly in vitro with little
or no apparent change in their plasticity. In one study,
human neural progenitors isolated from embryonic fore-
brain were expanded for up to a year in culture using
Epidermal Growth Factor (EGF) Fibroblast Growth Factor
(FGF) and leukaemia inhibitory factor (LIF). Subsequent
injection of these cell lines into the developing rat brain
showed extensive migration and integration.98,99
Clinical use of fetal tissue for stem-cell transplantation
is made difficult by ethical constraints. Confronted with the
spectre of couples conceiving for the sole purpose of
obtaining aborted brain tissue for the treatment either of
a parent or of an afflicted sibling, scientists have turned to
less conventional sources for NSCs. Indeed, investigators
have claimed to isolate functional NSCs from adult post-
mortem brain tissue as late as 5 days after death.100
Al-
though it is suspected that adult NSCs have a more limited
ability than fetal NSCs to form all the neural subtypes, they
might have a broader potential than first thought.
Stem cells from non-neural tissues
Recent studies have suggested that mesenchymal stem cells
(MSCs) from certain adult and fetal tissues have the potential
to exhibit phenotypic characteristics of cells not expected
within the tissue of origin,101,102
including neural pheno-
types. These tissues include bone marrow,103
peripheral
blood,104e106
umbilical cord blood107e109
and umbilical cord
matrix (Wharton’s jelly) cells.110,111
As well as representing
a plentiful, ethically acceptable and easily accessible source
of neural tissue for CNS repair, these cells could potentially
be used autologously, thereby reducing the risk of tissue re-
jection. To date, however, little is known about the sour-
ce(s), frequency and characteristics of cells with the
potential to adopt neural lineages. Although there is cur-
rently no specific antigenic marker for these cells, they are
known to express CD105, CD73, STRO-1 and proly-4-hydroxy-
lase. They do not express markers of the haematopoietic lin-
eage, such as CD34 and CD45.61
They also have osteogenic,
adipogenic and chondrogenic differentiation potential.
Wharton’s jelly (WJ) is the gelatinous connective
tissue that constitutes the umbilical cord. It is composed
of myofibroblast-like stromal (Wharton’s jelly) cells,
collagen fibres and proteoglycans.112
WJ cells express
several stem-cell markers, including c-kit and Oct-4, as
well as telomerase, an enzyme that inhibits cell senes-
cence by maintaining telomere length. They also seem
to have neurogenic potential.110
WJ cells have been
shown to survive for at least 6 weeks following intracere-
bral transplantation or systemic infusion without the need
for immunosuppression of the host rat. Cells labelled with
enhanced green fluorescent protein (eGFP) migrated ex-
tensively after implantation and co-expressed neuronal
filament 70 (NF70).111
To date, no electrophysiological
confirmation of neuronal differentiation has been re-
ported for WJ cells and, similarly, no behavioural assess-
ment of animals transplanted with WJ cells has yet been
264 R. Vawda et al.
7. published, because they have not yet been used in any
disease model.
The generation of neural cells from bone marrow could
be due either to the presence of a minute subpopulation of
highly pluripotent cells in the marrow or to the reprogram-
ming (trans- or de-differentiation) of an already committed
blood progenitor. Indeed, Verfaillie’s group has described
the ‘multipotent adult progenitor cell’ (MAPC) as a bone-
marrow-derived cell with multitissue potential,113
including
neural lineages. When transplanted, these cells have been
shown to ameliorate neurological deficits in a rat model
of cerebral ischaemia.114
There are several reports of non-neural stem cells
undergoing transdifferentiation to a pro-neural form. Al-
though controversial, much of the transdifferentiation data
are tantalizing and are not easily explained by the fusion of
stem cells with more differentiated ones. However, no
study has yet isolated, purified or expanded neural-like
cells from bone marrow or Wharton’s jelly, and many have
used non-physiological (toxic and carcinogenic) stimuli to
induce or promote the emergence of neural-like cells,
which would limit their clinical application. The use of
substances toxic to cells can cause them to react non-
specifically with a range of antigenic neural markers.115
An-
other problem with the majority of transdifferentiation
studies is that the starting population of cells is heteroge-
neous and there remains the possibility that small numbers
of contaminating neural cells, or more multipotent cells,
account for the result.
MSCs offer a number of advantages over NSCs and ES
cells for clinical implantation:
They are more easily and ethically isolated than NSCs.
They have a greater ability to home in on the brain than
NSCs after intravenous infusion, although no systematic
comparison has yet been carried out.116e119
They negate the need for immunosuppression in the case
of autologous transplants and possibly even in the case of
heterologous transplants.111,120,121
The same might not
be true of NSCs,122,123
MSCs have already been used in
several clinical trials of autologous transplantation for
a wide range of conditions and were found to be well tol-
erated with minimal side-effects.124
They present fewer ethical constraints than NSCs iso-
lated from human fetal CNS tissue and human ES cells.
They are likely to be confronted with fewer regulatory ob-
stacles.Autologous transplantations ofbonemarrowstem
cells (BMSCs) are already possible and such cells from
postnataltissueopenupthepossibilityofusingautologous
transplants to treat neurodegenerative conditions.103
They have a greater differentiation potential than
NSCs, which might be restricted to neural fates.125e130
There are a number of possible drawbacks to using non-
neural sources of neural-like cells for intracerebral implan-
tation. Tumour formation after BM cell intracerebral
implantation in rats has been reported (D. Bonnet, personal
communication, November 2003). So far, there has been
only one report of tumour formation following NSC implan-
tation.131
Furthermore, neural-like cells derived from non-
neural tissue might not be able to respond appropriately to
positional signals within the recipient brain, as indicated by
their presence in inappropriate areas [H. Mehmet, personal
communication, November 2003]. This latter observation
contrasts with published observations of the fate of do-
nor-derived BM cells in the human CNS,132
and of BM-de-
rived MAPCs implanted into blastocyst-stage mouse
embryos,133
which have indicated that they might respond
to local positional and migrational signals within the recip-
ient brain. These discrepancies highlight the need for cau-
tion during the design of transplantation studies and the
subsequent interpretation of results.
Immortalized cell lines
As an alternative to fetal tissue, immortalized cell lines
have been used in animal models of brain injury. Neurons
grafted from a human teratocarcinoma cell line into rats
with focal ischaemia resulted in histological integration and
functional improvement,134
as did grafting a hippocampal
neuroepithelial cell line into damaged hippocampus in the
mouse.135
A number of studies have also demonstrated
the successful transplantation of oligodendrocyte progeni-
tor cell lines for demyelinating diseases, including experi-
mental autoimmune encephalomyelitis136
and ethidium
bromide-induced demyelinating lesions in the spinal
cord.137
There are, however, considerable fears that im-
mortalized cell lines are prone to tumourogenesis and
that they are unable to reconstitute the wide variety of
cell types lost in cerebral injury. This makes them of only
limited use in clinical applications.
Perinatal clinical applications for stem
cell therapy
Perinatal H/I and TBI
Theaim ofanytherapy after a perinatal braininjury,whether
it be H/I or TBI, is functional repair. For this to occur it is
necessary for new projection neurons to be generated in
addition to new interneurons and glial subtypes.
There is increasing evidence to support the existence of
endogenous compensatory mechanisms, which are acti-
vated in response to injury and disease.138e140
For example,
a low level of ongoing neurogenesis has recently been shown
to occur in the adult mammalian striatum.88
Similarly, tar-
geted apoptotic degeneration of murine cortical neurons
has been shown to trigger the formation of new neocortical
projection neurons, whose axons extend into the thala-
mus,141
and a similar process has been observed following is-
chaemia, which promotes neurogenesis in the rat SVZ, with
newly generated neurons migrating into the striatum where
they mature into spinal striatal neurons.142,143
In other studies, neurogenesis has been demonstrated in
models of newborn hypoxic ischaemic brain injury,144
and
similarly active neurogenesis has been demonstrated in
aged and young rats following stroke.145
SVZ cell prolifera-
tion is enhanced further in rats housed in an enriched envi-
ronment following stroke.146
Similar observations have been made in demyelinating
diseases, such as multiple sclerosis (MS), which might have
Stem cells for brain injuries 265
8. implications for ischaemic white-matter injury in the
neonate. In chronic MS lesions, the presence of NG2þ
premyelinating oligodendrocytic progenitors has been re-
ported,147,148
although the relationship between endoge-
nous gliogenesis and remission is still unclear.
Studies using BrdU labelling of proliferating cells, whose
migration was confirmed by retroviral tracing, have dem-
onstrated the expansion and subsequent differentiation of
endogenous neural precursors following experimental
stroke.149
Similarly, NSC proliferation has been found to in-
crease ten-fold in the subgranular zone of the dentate gy-
rus after global ischaemia in the gerbil.150
Endogenous
repair in response to stroke can also involve the prolifera-
tion of neural progenitor cells in the SVZ. Following middle
cerebral artery occlusion, injection of BrdU specifically la-
belled astrocytes in the ependymal and subependymal
layers that later acquired the characteristic antigenic
markers of neurons after injury.151
In a separate model em-
ploying chemically induced seizures in the rodent, a pro-
nounced increase in the generation of new neuronal
precursors in the subventricular zone (SVZ) and their subse-
quent migration and integration towards the olfactory bulb
was reported.152,153
While it has been proposed that ischae-
mia-induced neurogenesis might contribute to the specific
recovery of memory function lost following injury, a high
proportion of the dividing cells are lost over the weeks after
injury. Current evidence suggests that SVZ-derived cells
that migrate in response to injury either form interneu-
rons154
or do not survive long term.144,155
The failure of the SVZ to repopulate the brain might
reflect the maturational state of the perinatal brain. As
reviewed earlier, the projection neurons of the brain are
descended from radial cells, which are also the essential
physical scaffold neurons require to migrate from their
periventricular origin into the neocortex. In late develop-
ment, the radial glial scaffold collapses as most of these
radial glial cells differentiate into astrocytes,156
potentially
blocking migration of any newly generated pyramidal neu-
rons. A recent study by Plane et al.155
showed Dcxþ cells
adjacent to GFAP-positive astrocytes and suggested that
they were using these glial cells to support their migration.
Also, Fagel et al.157
reported a similar phenomenon where
the migrating cells were closely associated with GFAP-pos-
itive cells. Ganat et al.158
had shown earlier that there was
an increase in cells expressing markers associated with ra-
dial glia after chronic hypoxia and, given the role of the ra-
dial cells in both neurogenesis and migration, suggested
that these cells were participating in the regeneration of
neurons lost during the insult. However, they also failed
to find any of their newly generated neurons expressing
projection neuron markers. To date, the only experimental
paradigm where new projection neurons are generated af-
ter cerebral injury is in the targeted cell ablation model
pioneered by Dr Jeffrey Macklis and colleagues. Their stud-
ies have demonstrated that the mature brain retains the
capacity to generate new projection neurons, but that their
production occurs only under highly controlled conditions in
which neuroinflammation is curtailed.141
Given the limited replacement of brain cells that occurs
naturally, it is likely that the numbers of endogenous pre-
cursors available are insufficient to fully repopulate the
brain. Moreover, given that pyramidal cells are not replaced
after ischaemic insults, strategies must be formulated to
expand the regenerative potential of the somatic NSCs, and/
or exogenous stem-cell transplantation might be necessary.
Issues related to where these exogenous cells are obtained,
how and where they will be transplanted, and whether they
will be retained in vivo need to be considered. Given their
ability to migrate extensively and integrate after trans-
plantation into the brain,98,99,159
it might be possible to use
neural stem progenitors (NSPs) derived from fetal sources,
but these cells are in very limited supply. Accordingly, ES-
cell-derived neural precursors represent the most feasible
source of cells for transplantation, because they also effec-
tively migrate and differentiate into mature cell types after
implantation.160
Ironically, obtaining neural precursors for
transplantation might be the least difficult hurdle towards
implementing brain cell replacement. Transplanting new
stem cells into the brain will not guarantee successful repair.
The success of any attempted repair will depend on the se-
verity of the insult, the status of growth and survival factors,
and the ability of the transplanted cells to migrate, differen-
tiate and survive.
Another issue to be address is the massive cell death
after injury. Anti-apoptotic agents cannot address the
necrotic cell death that occurs immediately after an
ischaemic event, although they can decrease the amount
of delayed cell death in the subsequent hours, days and
weeks. In severe cases, however, the amount of damage
caused by the ischaemic event can be so extensive that
a lasting motor or cognitive deficit is sustained. Despite the
established knowledge that widespread cell death follows
such cerebrovascular incidents, pharmacological interven-
tions to minimize this (using anti-apoptotic agents) are not
common practice. In such cases, cell replacement would be
an ideal way to restore lost cells and function.
If stem cell therapy is to be implemented to repair the
infant brain after perinatal brain injury, it is likely that
certain groups of infants will benefit more than others.
Infants who are younger and have survived a less severe
insult might be better candidates for treatment than older
infants who have sustained a more serious insult. After an H/I
insult, for example, there is limited damage to neurons in the
brain of a premature infant, and one only needs to contem-
plate strategies to replace the deleted oligodendrocytes.
The somatic neural stem cells of the SVZ are fully competent
to generate oligodendrocytes, but they might require some
specification cues to perform appropriately. The provision of
specification cues for individual cell types would be a simpler
task than for multiple cells types, making the successful
treatment of a preterm infant via expansion and specifica-
tion of the endogenous stem cells a worthy goal.
By contrast, repairing the term infant brain that has
sustained neocortical damage, such as TBI or more severe
cases of H/I, will require a multilayered strategy. A strategy
similar to the following might be required for successful
treatment: the first step could be to suppress the pro-
duction of proinflammatory cytokines, which might inhibit
repair by stem cells and progenitors. Once that is achieved,
matched embryonic stem cells could be specified into radial
cells. Radial cells are a logical choice for transplantation
because they can function as both mediators for migration
and as bipotential precursors that are capable of generating
new projection neurons. Obviously, transplantation would
266 R. Vawda et al.
9. occur in conjunction with trophic factor supplementation.
The addition of growth factors such as FGF, EGF, LIF or
neuregulin161e163
would help to maintain the transplanted
radial cells as precursors and would alter the environment
in the brain to one that supports proliferation and differen-
tiation of progenitors. Once these precursors are trans-
planted, a period of time would need to pass to allow the
new cells to migrate, differentiate and form new connec-
tions. During and after this period, it would be necessary
to continue the supply of trophic factors and cytokines to
promote the proliferation of endogenous stem cells as
well as the transplanted ones. This supplementation would
also include factors to suppress astrogliogenesis to ensure
that cells are differentiating into necessary cells types
(i.e. neurons and oligodendrocytes). This supplementation
would probably need to be continued long term, with inten-
sive physical therapy to stimulate and maintain newly
formed cells and their connections. Indeed, even with ad-
vanced imaging methods, it remains a challenge to give
an early estimate of long-term prognosis in moderately af-
fected infants, and thus difficult to define a population for
study so as to be confident of outcome differences. The na-
ture of the term brain and the complexity of this treatment
makes the goal of repairing the term infant brain a more
difficult prospect than regenerating the preterm infant
brain, however advances in the understanding of stem
cell biology might make it achievable.
Metabolic brain diseases
One of the major advantages of considering perinatal cell
therapy for inborn errors of metabolism is that, if the
diagnosis is known, treatment could be commenced early to
prevent or minimize ongoing brain damage or deteriora-
tion. It is important to recognize, however, that the
majority of infants with metabolic diseases (frequently
autosomal recessive) do not have affected parents and so
treatment before the onset of symptoms or manifestations,
especially in utero, would not generally be possible. There
are other important issues to take into account. First, it
could be argued that metabolic diseases are multiorgan
diseases and should therefore be treated with global cell
therapy, such as bone marrow transplantation (BMT),
although this approach might have little impact on neuro-
logical deterioration. One example of this is the treatment
of metachromatic leukodystrophy (arylsulfatase deficiency)
with BMT, where it was found that lipid storage was
improved only in the kidney and liver of transplanted
animals, and that neuronal damage in the brain was as
severe as in the untreated animals.164
Second, in a given metabolic disorder where the major-
ity of cells are likely to be affected, it would be unlikely
that a cell replacement strategy would be curative. Cell
replacement therapy might attenuate the clinical course of
the disease and this has been demonstrated with oligoden-
drocyte progenitor cell therapy in metachromatic leuko-
dystrophy.165
However, stem cells could be used as vehicles
to deliver a missing or aberrant gene or protein, or simply
to generate trophic support for endogenous cells to slow
their degeneration.
Also, cell therapy would have to be designed in such a way
that grafted cells would escape the pathological processes
affecting host cells. Already, several researchers have
examined NSC therapy in models with inborn errors of
metabolism with mixed results. Meng et al. investigated
the possibility of using NSC in the treatment of metabolic
brain disease in a murine model of mucopolysaccharidosis
type VII.166
This condition arises from a defect in the alpha-
glucuronidase gene and results in lysosomal accumulation of
glycosaminoglycans in the brain, with subsequent neurode-
generation. In this study, NSCs were modified to overexpress
the missing enzyme (alpha-glucuronidase) and transplanted
into the cerebral ventricles of newborn affected mice.
These NSCs migrated widely and produced large quantities
of alpha-glucuronidase, resulting in a dramatic clearance
of the lysosomal accumulation in host cells to near normal
levels. Such experiments prove e in principle e that NSCs
can be used for gene delivery in genetic deficiency disorders.
One downside in this experiment was that graft survival was
limited by apoptotic cell death of the grafted cells, limiting
the duration of the benefit achieved.
Newborn white-matter disease
Although in the majority of CNS diseases a number of
different cell types are affected, cell replacement therapy
has been most successfully used in models where damage to
a single cell type is predominant. One example of this is
white-matter disease and, indeed, there are already
several rodent models with specific abnormalities in oligo-
dendrocytes e the myelin-forming cells of the CNS. As well
as demonstrating proof of principle, these models will
provide useful prototypes for perinatal therapy. There is
accumulating evidence that, although periventricular leu-
komalacia is becoming rare, brain injury or abnormalities
found in the majority of survivors of extremely preterm
birth remain predominantly in white matter and involve
oligodendrocyte precursor loss.
Magnetic resonance imaging studies have confirmed
involvement of the white matter21,22
and in vitro data
also suggest that oligodendrocyte precursors, abundant in
the preterm brain, are very much more vulnerable to a vari-
ety of stressors compared to mature oligodendrocytes.35
Oligodendrocyte death or maldevelopment may be a pri-
mary event in preterm brain injury. Despite the distance
between the theory and clinical practice of NSC trans-
plants, studies examining oligodendrocyte replacement in
demyelinating models of multiple sclerosis have provided
some encouraging results; however, no work is currently
underway in preterm brain injury.
If cell-based therapy is to be considered for these infants,
better tools will be needed to estimate long-term neuro-
developmental outcome in the perinatal period, so as to
optimize patient selection, and a better understandingof the
pathogenesis of the condition is necessary. At present,
neither of these obstacles is close to being overcome.
Future perspectives
Many issues remain to be clarified about stem-cell trans-
plantation into injured or diseased brains, including the
fundamental one as to which cell sources are best suited for
therapy.167
The pathogenesis of many CNS disorders is not
Stem cells for brain injuries 267
10. fully understood and this precludes the directed use of
stem cells for restorative therapy in many cases. In an ideal
world, one would be able to stimulate the proliferation and
appropriate differentiation of endogenous stem cells. In-
deed, a number of gene-delivery-based therapies might
work, at least in part, through this approach. Early experi-
ments in stem-cell transplantation suggested that embry-
onic cells are significantly more plastic than adult ones.
Any research that relies on fetal tissues (especially when
derived by therapeutic cloning) will be ethically controver-
sial. Consequently, efforts should also focus on adult sour-
ces of stem cells for neural cell replacement. Although
research has indicated that adult NSCs possess a broader
developmental potential than was first thought, they do
have a more limited lifespan than ES or fetal-derived cells.
Whether the starting material is embryonic, fetal or adult-
derived, cell replacement strategies must also contend
with the influence of environmental signals. In several
models of adult brain repair, transplants are prone to apo-
ptosis for prolonged periods after transfer and so clinical
improvement might only be temporary.69
Considerable
work is therefore needed to identify the triggers for specific
neural cell survival and integration, and to further deter-
mine how the environment of the injured brain may be ma-
nipulated to become more permissive for effective repair.
References
*1. Vannucci RC, Vannucci SJ. Perinatal hypoxic-ischemic brain
damage: evolution of an animal model. Developmental Neu-
roscience 2005;27(2e4):81e6.
2. Hill A. Current concepts of hypoxic-ischemic cerebral injury
in the term newborn. Pediatric Neurology 1991;7(5):317e25.
3. Espinoza MI, Parer JT. Mechanisms of asphyxial brain damage,
andpossiblepharmacologicinterventions,inthefetus.American
Journal Of Obstetrics Gynecology 1991;164(6 Pt 1):1582e9.
4. Raichle ME. The pathophysiology of brain ischemia. Annals of
Neurology 1983;13(1):2e10.
5. Hagberg H, Thornberg E, Blennow M, et al. Excitatory amino
acids in the cerebrospinal fluid of asphyxiated infants: rela-
tionship to hypoxic-ischemic encephalopathy. Acta Paediatr-
ica 1993;82(11):925e9.
6. Puka-Sundvall M, Gajkowska B, Cholewinski M, Blomgren K,
Lazarewicz JW, Hagberg H. Subcellular distribution of cal-
cium and ultrastructural changes after cerebral hypoxia-is-
chemia in immature rats. Developmental Brain Research
2000;123:31e41.
7. Puka-Sundvall M, Sandberg M, Hagberg H. Brain injury after
hypoxia-ischemia in newborn rats: relationship to extracellu-
lar levels of excitatory amino acids and cysteine. Brain
Research 1997;750:325e8.
8. Blomgren K, Zhu C, Wang X, et al. Synergistic activation of
caspase-3 by m-calpain after neonatal hypoxia-ischemia:
a mechanism of ‘‘pathological apoptosis’’? Journal of Biolog-
ical Chemistry 2001;276(13):10191e8.
9. Gill R, Soriano M, Blomgren K, et al. Role of caspase-3 acti-
vation in cerebral ischemia-induced neurodegeneration in
adult and neonatal brain. Journal of Cerebral Blood Flow
and Metabolism 2002;22(4):420e30.
10. Wang X, Karlsson JO, Zhu C, Bahr BA, Hagberg H, Blomgren K.
Caspase-3 activation after neonatal rat cerebral hypoxia-
ischemia. Biology of The Neonate 2001;79(3e4):172e9.
11. Zhu C, Wang X, Hagberg H, Blomgren K. Correlation between
caspase-3 activation and three different markers of DNA
damage in neonatal cerebral hypoxia-ischemia. Journal of
Neurochemistry 2000;75(2):819e29.
*12. Romanko MJ, Levison SW, Rothstein RP. Neural stem cells in
the subventricular zone are resilient to hypoxia/ischemia
whereas progenitors are vulnerable. Journal of Cerebral
Blood Flow and Metabolism 2004;24(7):814e25.
13. Hu BR, Liu CL, Ouyang Y, Blomgren K, Siesjo BK. Involvement
of caspase-3 in cell death after hypoxia-ischemia declines
during brain maturation. Journal of Cerebral Blood Flow
and Metabolism 2000;20(9):1294e300.
14. Northington FJ, Ferriero DM, Flock DL, Martin LJ. Delayed neu-
rodegeneration in neonatal rat thalamus after hypoxia-ische-
mia is apoptosis. Journal of Neuroscience 2001;21(6):1931e8.
15. Northington FJ, Ferriero DM, Martin LJ. Neurodegeneration
in the thalamus following neonatal hypoxia-ischemia is
programmed cell death. Developmental Neuroscience 2001;
23(3):186e91.
16. Ness JK, Wood TL. Insulin-like growth factor I, but not neuro-
trophin-3, sustains Akt activation and provides long-term
protection of immature oligodendrocytes from glutamate-
mediated apoptosis. Molecular and Cellular Neuroscience
2002;20(3):476e88.
17. Vannucci RC. Experimental biology of cerebral hypoxia-is-
chemia: relation to perinatal brain damage. Pediatric Re-
search 1990;27(4 Pt 1):317e26.
18. Hammerman C, Kaplan M. Ischemia and reperfusion injury.
The ultimate pathophysiologic paradox. Clinics in Perinatol-
ogy 1998;25(3):757e77.
19. Foster-Barber A, Dickens B, Ferriero DM. Human perinatal as-
phyxia: correlation of neonatal cytokines with MRI and out-
come. Developmental Neuroscience 2001;23(3):213e8.
20. Oygur N, Sonmez O, Saka O, Yegin O. Predictive value of
plasma and cerebrospinal fluid tumour necrosis factor-alpha
and interleukin-1 beta concentrations on outcome of full
term infants with hypoxic-ischaemic encephalopathy. Ar-
chives of Disease in Childhood Fetal and Neonatal Edition
1998;79(3):F190e3.
21. Counsell SJ, Rutherford MA, Cowan FM, Edwards AD. Mag-
netic resonance imaging of preterm brain injury. Archives
of Disease in Childhood Fetal and Neonatal Edition 2003;
88(4):F269e74.
22. Maalouf EF, Duggan PJ, Rutherford MA. Magnetic resonance
imaging of the brain in a cohort of extremely preterm in-
fants. Journal of Pediatrics 1999;135(3):351e7.
23. Inder T, Huppi PS, Zientara GP. Early detection of periven-
tricular leukomalacia by diffusion-weighted magnetic reso-
nance imaging techniques. Journal of Pediatrics 1999;
134(5):
631e4.
24. Inder TE, Huppi PS, Warfield S. Periventricular white matter
injury in the premature infant is followed by reduced cere-
bral cortical gray matter volume at term. Annals of Neurol-
ogy 1999;46(5):755e60.
25. Peterson BS, Vohr B, Staib LH. Regional brain volume abnor-
malities and long-term cognitive outcome in preterm infants.
Journal of the American Medical Association 2000;284(15):
1939e47.
26. Peterson BS, Anderson AW, Ehrenkranz R. Regional brain vol-
umes and their later neurodevelopmental correlates in term
and preterm infants. Pediatrics 2003;111(5 Pt 1):939e48.
27. Mcquillen PS, Sheldon RA, Shatz CJ, Ferriero DM. Selective
vulnerability of subplate neurons after early neonatal
hypoxia-ischemia. Journal of Neuroscience 2003;23(8):
3308e15.
28. Sizonenko SV, Sirimanne E, Mayall Y, Gluckman PD, Inder T,
Williams C. Selective cortical alteration after hypoxic-ische-
mic injury in the very immature rat brain. Pediatric Research
2003;54(2):263e9.
268 R. Vawda et al.
11. 29. Sheldon RA, Chuai J, Ferriero DM. A rat model for hypoxic-
ischemic brain damage in very premature infants. Biology
of the Neonate 1996;69(5):327e41.
30. Curristin SM, Cao A, Stewart WB. Disrupted synaptic develop-
ment in the hypoxic newborn brain. Proceedings of the Na-
tional Academy of Science of the United States of America
2002;99(24):15729e34.
31. Rothstein RP, Levison SW. Gray matter oligodendrocyte pro-
genitors and neurons die caspase-3 mediated deaths subse-
quent to mild perinatal hypoxic/ischemic insults.
Developmental Neuroscience 2005;27(2e4):149e59.
32. Greisen G. Cerebral blood flow in preterm infants during the
first week of life. Acta Paediatrica Scandinavica 1986;75(1):
43e51.
33. Lou HC, Han BH, Luo NL, et al. Pressure passive cerebral
blood flow and breakdown of the bloodebrain barrier in ex-
perimental fetal asphyxia. Acta Paediatrica Scandinavica
1979;68(1):
57e63.
34. Back SA, Han BH, Luo NL. Selective vulnerability of late oli-
godendrocyte progenitors to hypoxia-ischemia. Journal of
Neuroscience 2002;22(2):455e63.
35. Ness JK, Romanko MJ, Rothstein RP, Wood TL, Levison SW.
Perinatal hypoxia-ischemia induces apoptotic and excito-
toxic death of periventricular white matter oligodendro-
cyte progenitors. Developmental Neuroscience 2001;23(3):
203e8.
36. Ness JK, Mitchell NE, Wood TL. IGF-I and NT-3 signaling path-
ways in developing oligodendrocytes: differential regulation
and activation of receptors and the downstream effector
Akt. Developmental Neuroscience 2002;24(5):437e45.
37. Back SA, Gan X, Li Y, Rosenberg PA, Volpe JJ. Maturation-de-
pendent vulnerability of oligodendrocytes to oxidative
stress-induced death caused by glutathione depletion. Jour-
nal of Neuroscience 1998;18(16):6241e53.
38. Keenan HT, Bratton SL. Epidemiology and outcomes of pedi-
atric traumatic brain injury. Developmental Neuroscience
2006;28(4e5):256e63.
*39. Tasker RC. Changes in white matter late after severe trau-
matic brain injury in childhood. Developmental Neuroscience
2006;28(4e5):302e8.
40. Bayir H, Kochanek PM, Kagan VE. Oxidative stress in imma-
ture brain after traumatic brain injury. Developmental Neu-
roscience 2006;28(4e5):420e31.
41. Robertson CL, Soane L, Siegel ZT, Fiskum G. The potential
role of mitochondria in pediatric traumatic brain injury. De-
velopmental Neuroscience 2006;28(4e5):432e46.
42. Thompson HJ, Lifshitz J, Marklund N, et al. Lateral fluid per-
cussion brain injury: a 15-year review and evaluation. Jour-
nal of Neurotrauma 2005;22(1):42e75.
43. Cortez SC, Mcintosh TK, Noble LJ. Experimental fluid percus-
sion brain injury: vascular disruption and neuronal and glial
alterations. Brain Research 1989;482(2):271e82.
44. Hicks R, Soares H, Smith D, McIntosh T. Temporal and spatial
characterization of neuronal injury following lateral fluid-
percussion brain injury in the rat. Acta Neuropathologica
(Berlin) 1996;91(3):236e46.
45. Rink A, Fung KM, Trojanowski JQ, Lee VM, Neugebauer E,
McIntosh TK. Evidence of apoptotic cell death after experi-
mental traumatic brain injury in the rat. American Journal
of Pathology 1995;147(6):1575e83.
46. Conti AC, Raghupathi R, Trojanowski JQ, McIntosh TK. Exper-
imental brain injury induces regionally distinct apoptosis
during the acute and delayed post-traumatic period. Journal
of Neuroscience 1998;18(15):5663e72.
47. Smith DH, Chen XH, Pierce JE, et al. Progressive atrophy and
neuron death for one year following brain trauma in the rat.
Journal of Neurotrauma 1997;14(10):715e27.
*48. Pullela R, et al. Traumatic injury to the immature brain re-
sults in progressive neuronal loss, hyperactivity and delayed
cognitive impairments. Developmental Neuroscience 2006;
28(4e5):396e409.
49. Weller S, Gould SJ, Valle D. Peroxisome biogenesis disorders.
Annual Review of Genomics and Human Genetics 2003;4:
165e211.
50. Oglesbee D. An overview of peroxisomal biogenesis disor-
ders. Molecular Genetics and Metabolism 2005;84(4):
299e301.
51. Powers JM. Demyelination in peroxisomal diseases. Journal
of the Neurological Sciences 2005;228:206e7.
52. Ginzburg L, Kacher Y, Futerman AH. The pathogenesis of gly-
cosphingolipid storage disorders. Seminars in Cell Develop-
mental Biology 2004;15:417e31.
53. Futerman AH, Van meer G. The cell biology of lysosomal stor-
age disorders. Nature Reviews, Molecular Cell Biology 2004;
5:554e65.
54. Gallo V, de Vellis J. Preface: white matter disorders. Mental
Retardation and Developmental Disabilities Research
Reviews 2006;12(2):83e4.
*55. Sen E, Levison SW. Astrocytes and developmental white mat-
ter disorders. Mental Retardation and Developmental
Disabilities Research Reviews 2006;12(2):97e104.
56. Van Der Knaap MS, Pronk JC, Scheper GC. Vanishing white
matter disease. Lancet Neurology 2006;5(5):413e23.
57. Kumar S, Mattan NS, De Vellis J. Canavan disease: a white
matter disorder. Mental Retardation and Developmental Dis-
abilities Research Reviews 2006;12(2):157e65.
58. Gorospe JR, Maletkovic J. Alexander disease and megalence-
phalic leukoencephalopathy with subcortical cysts: leuko-
dystrophies arising from astrocyte dysfunction. Mental
Retardation and Developmental Disabilities Research Re-
views 2006;12:113e22.
59. Counsell SJ, Allsop JM, Harrison MC, et al. Diffusion-weighted
imaging of the brain in preterm infants with focal and diffuse
white matter abnormality. Pediatrics 2003;112(1 Pt 1):1e7.
60. Thomson JA, Itskovitz-Eldor J, Shapiro SS, et al. Embryonic
stem cell lines derived from human blastocysts. Science
1998;282(5391):1145e7.
61. Minguell JJ, Erices A, Conget P. Mesenchymal stem cells.
Experimental Biology and Medicine (Maywood) 2001;
226(6):507e20.
62. Bain G, Kitchens D, Yao M, Huettner JE, Gottlieb DI. Embry-
onic stem cells express neuronal properties in vitro. Develop-
mental Biology 1995;168(2):342e57.
63. Brustle O, Spiro AC, Karram K, Choudhary K, Okabe S,
McKay RD. In vitro-generated neural precursors participate
in mammalian brain development. Proceedings of the Na-
tional Academy of Sciences of the United States of America
1997;94(26):14809e14.
64. Carpenter MK, Inokuma MS, Denham J, Mujtaba T, Chiu CP,
Rao MS. Enrichment of neurons and neural precursors from
human embryonic stem cells. Experimental Neurology
2001;172(2):383e97.
65. Reubinoff BE, Itsykson P, Turetsky T, et al. Neural progenitors
from human embryonic stem cells. Nature Biotechnology
2001;19(12):1134e40.
66. Flax JD, Aurora S, Yang C, et al. Engraftable human neural
stem cells respond to developmental cues, replace neurons,
and express foreign genes. Nature Biotechnology 1998;
16(11):1033e9.
67. Brustle O, Jones KN, Learish RD, et al. Embryonic stem cell-
derived glial precursors: a source of myelinating transplants.
Science 1999;285(5428):754e6.
68. Liu S, Qu Y, Stewart TJ, et al. Embryonic stem cells differ-
entiate into oligodendrocytes and myelinate in culture and
after spinal cord transplantation. Proceedings of the
Stem cells for brain injuries 269
12. National Academy of Sciences of the United States of
America 2000;97(11):6126e31.
69. Svendsen CN, Clarke DJ, Rosser AE, Dunnett SB. Survival
and differentiation of rat and human epidermal growth
factor-responsive precursor cells following grafting into
the lesioned adult central nervous system. Experimental
Neurology 1996;137(2):376e88.
70. Mcdonald JW, Liu XZ, Qu Y, et al. Transplanted embryonic
stem cells survive, differentiate and promote recovery in in-
jured rat spinal cord. Nature Medicine 1999;5(12):1410e2.
71. Misson JP, Austin CP, Takahashi T, Cepko CL, Caviness Jr VS.
The alignment of migrating neural cells in relation to the mu-
rine neopallial radial glial fiber system. Cerebral Cortex
1991;1(3):221e9.
72. Rakic P. Neuron-glia relationship during granule cell migra-
tion in developing cerebellar cortex. A Golgi and electronmi-
croscopic study in Macacus Rhesus. Journal of Comparative
Neurology 1971;141(3):283e312.
*73. Angevine JB, Sidman RL. Autoadiographic study of cell migra-
tion during histogenesis of cerebral cortex in the mouse.
Nature 1961;192:766e8.
74. Gray GE, Sanes JR. Migratory paths and phenotypic choices
of clonally related cells in the avian optic tectum. Neuron
1991;6:211e25.
75. Campbell K, Gotz M. Radial glia: multi-purpose cells for ver-
tebrate brain development. Trends in Neurosciences 2002;
25(5):235e8.
76. Hartfuss E, et al. Characterization of CNS precursor subtypes
and radial glia. Developmental Biology 2001;229(1):15e30.
77. Malatesta P, Hartfuss E, Gotz M. Isolation of radial glial cells
by fluorescent-activated cell sorting reveals a neuronal line-
age. Development e Supplement 2000;127(24):5253e63.
78. Noctor SC, Flint AC, Weissman TA, Dammerman RS,
Kriegstein AR. Neurons derived from radial glial cells estab-
lish radial units in neocortex. Nature 2001;409(6821):
714e20.
79. Globus JH, Kuhlenbeck H. Subependymal cell plate (matrix)
and its relation to brain tumors of ependymal type. Journal
of Neuropathology 1944;3:1e35.
80. Thomaidou D, Mione MC, Cavanagh JFR, Parnavelas JG. Apo-
ptosis and its relation to the cell cycle in the developing ce-
rebral cortex. Journal of Neuroscience 1997;17:1075e85.
81. Altman J. Proliferation and migration of undifferentiated
precursor cells in the rat during postnatal gliogenesis. Exper-
imental Neurology 1966;16(3):263e78.
82. Luskin MB. Restricted proliferation and migration of postna-
tally generated neurons derived from the forebrain subven-
tricular zone. Neuron 1993;11:173e89.
83. Levison SW, Chuang C, Abramson BJ, Goldman JE. The
migrational patterns and developmental fates of glial pre-
cursors in the rat subventricular zone are temporally reg-
ulated. Development 1993;119(3):611e22.
*84. Levison SW, Goldman JE. Both oligodendrocytes and astro-
cytes develop from progenitors in the subventricular zone
of postnatal rat forebrain. Neuron 1993;10(2):201e12.
85. Li G, Pleasure SJ. Morphogenesis of the dentate gyrus: what
we are learning from mouse mutants. Developmental Neuro-
science 2005;27(2e4):93e9.
86. Gould E, Reeves AJ, Graziano MSA, Gross CG. Neurogenesis in
the neocortex of adult primates. Science 1999;286(5439):
548e52.
87. Horner PJ, Power AE, Kempermann G, et al. Proliferation and
differentiation of progenitor cells throughout the intact adult
rat spinal cord. Journal of Neuroscience 2000;20(6):2218e28.
88. Zhao M, Momma S, Delfani K, et al. Evidence for neurogene-
sis in the adult mammalian substantia nigra. Proceedings of
the National Academy Science of the United States of Amer-
ica 2003;100(13):7925e30.
89. Dayer AG, Cleaver KM, Abouantoun T, Cameron HA. New ga-
baergic interneurons in the adult neocortex and striatum are
generated from different precursors. Journal of Cell Biology
2005;168(3):415e27.
90. Kornack DR, Rakic P. Cell proliferation without neurogenesis in
adult primate neocortex. Science 2001;294(5549):2127e30.
91. Carpenter MK, Cui X, Hu ZY, et al. In vitro expansion of a mul-
tipotent population of human neural progenitor cells. Exper-
imental Neurology 1999;158(2):265e78.
92. Piper DR, Mujtaba T, Keyoung H, et al. Identification and
characterization of neuronal precursors and their progeny
from human fetal tissue. Journal of Neuroscience Research
2001;66(3):356e68.
93. Mayerproschel M, Kalyani AJ, Mujtaba T, Rao MS. Isolation of
lineage-restricted neuronal precursors from multipotent
neuroepithelial stem cells. Neuron 1997;19(4):773e85.
94. Morrison SJ. Neuronal potential and lineage determination
by neural stem cells. Current Opinion in Cell Biology 2001;
13(6):666e72.
95. Morrison SJ. Neuronal differentiation: proneural genes in-
hibit gliogenesis. Current Biology 2001;11(9):R349e51.
96. Ostenfeld T, Joly E, Tai YT, et al. Regional specification of ro-
dent and human neurospheres. Developmental Brain Re-
search 2002;134(1e2):43e55.
97. Rao MS. Multipotent and restricted precursors in the central
nervous system. Anatomical Record 1999;257(4):137e48.
98. Englund U, Bjorklund A, Wictorin K. Migration patterns and
phenotypic differentiation of long-term expanded human neu-
ral progenitor cells after transplantation into the adult rat
brain. Developmental Brain Research 2002;134(1e2):123e41.
99. Englund U, Fricker-Gates RA, Lundberg C, Bjorklund A,
Wictorin K. Transplantation of human neural progenitor cells
into the neonatal rat brain: extensive migration and differ-
entiation with long-distance axonal projections. Experimen-
tal Neurology 2002;173(1):1e21.
*100. Palmer TD, Schwartz PH, Taupin P, Kaspar B, Stein SA,
Gage FH. Cell culture. Progenitor cells from human brain af-
ter death. Nature 2001;411(6833):42e3.
101. Howell JC, Lee WH, Morrison P, Zhong J, Yoder MC, Srour EF.
Pluripotent stem cells identified in multiple murine tissues.
Annals of the New York Academy of Sciences 2003;996:
158e73.
102. Meletis K, Frisen J. Blood on the tracks: a simple twist of
fate? Trends in Neuroscience 2003;26(6):292e6.
103. Sanchez-Ramos JR. Neural cells derived from adult bone
marrow and umbilical cord blood. Journal of Neuroscience
Research 2002;69(6):880e93.
104. Abuljadayel IS. Induction of stem cell-like plasticity in mono-
nuclear cells derived from unmobilised adult human periph-
eral blood. Current Medical Research Opinion 2003;19(5):
355e75.
105. Milhaud G. A human pluripotent stem cell in the blood of
adults: towards a new cellular therapy for tissue repair.
Bulletin de l’Academie Nationale de Medecine 2001;
185(3):567e77 [discussion 577e82].
106. Zhao Y, Glesne D, Huberman E. A human peripheral blood
monocyte-derived subset acts as pluripotent stem cells. Pro-
ceedings of the National Academy of Sciences of the United
States of America 2003;100(5):2426e31.
107. Ha Y, Choi JU, Yoon DH, et al. Neural phenotype expression
of cultured human cord blood cells in vitro. Neuroreport
2001;12(16):3523e7.
108. Ha Y, Lee JE, Kim KN, Cho YE, Yoon DH. Intermediate fila-
ment nestin expressions in human cord blood monocytes
(HCMNCs). Acta Neurochirurgica (Wien) 2003;145(6):483e7.
109. Lee OK, Kuo TK, Chen WM, Lee KD, Hsieh SL, Chen TH. Isola-
tion of multi-potent mesenchymal stem cells from umbilical
cord blood. Blood 2004;103(5):669e75.
270 R. Vawda et al.
13. 110. Mitchell KE, Weiss ML, Mitchell BM, et al. Matrix cells from
Wharton’s jelly form neurons and glia. Stem Cells 2003;
21(1):50e60.
111. Weiss ML, Mitchell KE, Hix JE, et al. Transplantation of por-
cine umbilical cord matrix cells into the rat brain. Experi-
mental Neurology 2003;182(2):288e99.
112. Kobayashi K, Kubota T, Aso T. Study on myofibroblast differ-
entiation in the stromal cells of Wharton’s jelly: expression
and localization of alpha-smooth muscle actin. Early Human
Development 1998;51(3):223e33.
113. Jiang Y, Vaessen B, Lenvik T, Blackstad M, Reyes M,
Verfaillie CM. Multipotent progenitor cells can be isolated
from postnatal murine bone marrow, muscle, and brain. Ex-
perimental Hematology 2002;30(8):896e904.
114. Zhao LR, Duan WM, Reyes M, Keene CD, Verfaillie CM,
Low WC. Human bone marrow stem cells exhibit neural phe-
notypes and ameliorate neurological deficits after grafting
into the ischemic brain of rats. Experimental Neurology
2002;174(1):11e20.
115. Lu P, Blesch A, Tuszynski MH. Induction of bone marrow stro-
mal cells to neurons: differentiation, transdifferentiation, or
artifact? Journal of Neuroscience Research 2004;77(2):
174e91.
116. Brazelton TR, Rossi FM, Keshet GI, Blau HM. From marrow to
brain: expression of neuronal phenotypes in adult mice. Sci-
ence 2000;290(5497):1775e9.
117. Chu K, Kim M, Jeong SW, Kim SU, Yoon BW. Human neural
stem cells can migrate, differentiate, and integrate after in-
travenous transplantation in adult rats with transient fore-
brain ischemia. Neuroscience Letters 2003;343(2):129e33.
118. Eglitis MA, Mezey E. Hematopoietic cells differentiate into
both microglia and macroglia in the brains of adult mice.
Proceedings of the National Academy of Sciences of the
United States of America 1997;94(8):4080e5.
119. Mezey E, Chandross KJ, Harta G, Maki RA, McKercher SR.
Turning blood into brain: cells bearing neuronal antigens
generated in vivo from bone marrow. Science 2000;
290(5497):1779e82.
120. Le Blanc K. Immunomodulatory effects of fetal and adult
mesenchymal stem cells. Cytotherapy 2003;5(6):485e9.
121. Le Blanc K, Tammik C, Rosendahl K, Zetterberg E, Ringden O,
et al. Hla expression and immunologic properties of differen-
tiated and undifferentiated mesenchymal stem cells. Exper-
imental Hematology 2003;31(10):890e6.
122. Armstrong RJ, Tyers P, Jain M, et al. Transplantation of ex-
panded neural precursor cells from the developing pig ven-
tral mesencephalon in a rat model of Parkinson’s disease.
Experimental Brain Research 2003;151(2):204e17.
123. Hori J, Ng TF, Shatos M, Klassen H, Streilein JW, Young MJ. Neu-
ral progenitor cells lack immunogenicity and resistdestruction
as allografts. Stem Cells 2003;21(4):405e16.
124. Kassem M, Kristiansen M, Abdallah BM. Mesenchymal stem
cells: cell biology and potential use in therapy. Basic and
Clinical Pharmacology and Toxicology 2004;95(5):209e14.
125. Herzog EL, Chai L, Krause DS. Plasticity of marrow derived
stem cells. Blood 2003;102(10):3483e93.
126. Kicic A, Shen WY, Wilson AS, Constable IJ, Robertson T,
Rakoczy PE. Differentiation of marrow stromal cells into pho-
toreceptors in the rat eye. Journal of Neuroscience 2003;
23(21):7742e9.
127. Magrassi L. Differences and similarities among phenotypes of
mesenchymal and neural stem cells. Haematologica 2003;
88(2):121.
128. Magrassi L, Castello S, Ciardelli L, et al. Freshly dissociated
fetal neural stem/progenitor cells do not turn into blood.
Molecular and Cellular Neuroscience 2003;22(2):179e87.
129. Ortiz LA, Gambelli F, McBride C, et al. Mesenchymal stem cell
engraftment in lung is enhanced in response to bleomycin
exposure and ameliorates its fibrotic effects. Proceedings of
the National Academy of Sciences of the United States of
America 2003;100(14):8407e11.
130. Prockop DJ. Marrow stromal cells as stem cells for nonhema-
topoietic tissues. Science 1997;276(5309):71e4.
131. Zheng T, Steindler DA, Laywell ED. Transplantation of an in-
digenous neural stem cell population leading to hyperplasia
and atypical integration. Cloning Stem Cells 2002;4(1):3e8.
132. Mezey E, Key S, Vogelsang G, Szalayova I, Lange GD, Crain B.
Transplanted bone marrow generates new neurons in human
brains. Proceedings of the National Academy of Sciences of
the United States of America 2003;100(3):1364e9.
133. Keene CD, Ortiz-Gonzalez XR, Jiang Y, Largaespada DA,
Verfaillie CM, Low WC. Neural differentiation and incorpora-
tion of bone marrow-derived multipotent adult progenitor
cells after single cell transplantation into blastocyst stage
mouse embryos. Cell Transplant 2003;12(3):201e13.
134. Borlongan CV, Saporta S, Poulos SG, Othberg A, Sanberg PR.
Viability and survival of hNT neurons determine degree of
functional recovery in grafted ischemic rats. Neuroreport
1998;9(12):2837e42.
135. Sinden JD, Rashid Doubell F, Kershaw TR, et al. Recovery of
spatial learning by grafts of a conditionally immortalized hip-
pocampal neuroepithelial cell line into the ischaemia-le-
sioned hippocampus. Neuroscience 1997;81(3):599e608.
136. Tourbah A, Linnington C, Bachelin C, Avellana-Adalid V,
Wekerle H, Baron-Van Evercooren A. Inflammation pro-
motes survival and migration of the cg4 oligodendrocyte
progenitors transplanted in the spinal cord of both inflam-
matory and demyelinated EAE rats. Journal of Neuroscience
Research 1997;50(5):853e61.
137. Franklin RJ, Bayley SA, Blakemore WF. Transplanted Cg4
cells (an oligodendrocyte progenitor cell line) survive, mi-
grate, and contribute to repair of areas of demyelination
in X-irradiated and damaged spinal cord but not in normal
spinal cord. Experimental Neurology 1996;137(2):263e76.
138. Li Y, Chopp M. Temporal profile of nestin expression after
focal cerebral ischemia in adult rat. Brain Research 1999;
838:1e10.
139. Li Y, Chopp M, Powers C, Jiang N. Apoptosis and protein ex-
pression after focal cerebral ischemia in rat. Brain Research
1997;765(2):301e12.
140. Lindvall O, Mckay R. Brain repair by cell replacement and
regeneration. Proceedings of the National Academy of
Sciences of the United States of America 2003;100(13):
7430e1.
141. Magavi SS, Leavitt BR, Macklis JD. Induction of neurogene-
sis in the neocortex of adult mice. Nature 2000;405(6789):
951e5.
*142. Arvidsson A, Collin T, Kirik D, Kokaia Z, Lindvall O. Neuronal
replacement from endogenous precursors in the adult brain
after stroke. Nature Medicine 2002;8(9):963e70.
143. Parent JM, Vexler ZS, Gong C, Derugin N, Ferriero DM. Rat
forebrain neurogenesis and striatal neuron replacement af-
ter focal stroke. Annals of Neurology 2002;52(6):802e13.
144. Ong J, Plane JM, Parent JM, Silverstein FS. Hypoxic-ischemic
injury stimulates subventricular zone proliferation and neu-
rogenesis in the neonatal rat. Pediatric Research 2005;
58(3):600e6.
145. Darsalia V, Heldmann U, Lindvall O, Kokaia Z. Stroke-induced
neurogenesis in aged brain. Stroke 2005;36(8):1790e5.
146. Komitova M, Perfilieva E, Mattsson B, Eriksson PS,
Johansson BB. Enriched environment increases neural stem/-
progenitor cell proliferation and neurogenesis in the subven-
tricular zone of stroke-lesioned adult rats. Stroke 2005;
36(6):1278e82.
147. Chang A, Nishiyama A, Peterson J, Prineas J, Trapp BD. Ng2-
positive oligodendrocyte progenitor cells in adult human
Stem cells for brain injuries 271
14. brain and multiple sclerosis lesions. Journal of Neuroscience
2000;20(17):6404e12.
148. Chang A, Tourtellotte WW, Rudick R, Trapp BD. Premyelinat-
ing oligodendrocytes in chronic lesions of multiple sclerosis.
New England Journal of Medicine 2002;346(3):165e73.
149. Abe K. Therapeutic potential of neurotrophic factors and
neural stem cells against ischemic brain injury. [review]
[102 Refs]. Journal of Cerebral Blood Flow Metabolism
2000;20(10):1393e408.
150. Liu J, Solway K, Messing RO, Sharp FR. Increased neurogene-
sis in the dentate gyrus after transient global ischemia in
gerbils. Journal of Neuroscience 1998;18(19):7768e78.
151. Li Y, Chen J, Chopp M. Cell proliferation and differentiation
from ependymal, subependymal and choroid plexus cells in
response to stroke in rats. Journal of the Neurological Sci-
ences 2002;193(2):137e46.
152. Parent JM, Lowenstein DH. Seizure-induced neurogenesis:
are more new neurons good for an adult brain? Progress in
Brain Research 2002;135:121e31.
153. Parent JM, Valentin VV, Lowenstein DH. Prolonged seizures
increase proliferating neuroblasts in the adult rat subven-
tricular zone-olfactory bulb pathway. Journal of Neurosci-
ence 2002;22(8):3174e88.
154. Teramoto T, Qiu J, Plumier JC, Moskowitz MA. EGF amplifies
the replacement of parvalbumin-expressing striatal inter-
neurons after ischemia. Journal of Clinical Investigation
2003;111(8):1125e32.
155. Plane JM, Liu R, Wang TW, Silverstein FS, Parent JM. Neona-
tal hypoxic-ischemic injury increases forebrain subventricu-
lar zone neurogenesis in the mouse. Neurobiology Disease
2004;16(3):585e95.
156. Tramontin AD, Garcia-Verdugo JM, Lim DA, Alvarez-Buylla A.
Postnatal development of radial glia and the ventricular
zone (VZ): a continuum of the neural stem cell compart-
ment. Cerebral Cortex 2003;13(6):580e7.
157. Fagel DM, et al. Cortical neurogenesis enhanced by chronic
perinatal hypoxia. Experimental Neurology 2006;199(1):
77e91.
158. Ganat Y, Soni S, Chacon M, Schwartz ML, Vaccarino FM.
Chronic hypoxia up-regulates fibroblast growth factor ligands
in the perinatal brain and induces fibroblast growth factor-
responsive radial glial cells in the sub-ependymal zone. Neu-
roscience 2002;112(4):977e91.
159. Englund U, Bjorklund A, Wictorin K, Lindvall O, Kokaia M.
Grafted neural stem cells develop into functional pyramidal
neurons and integrate into host cortical circuitry. Proceed-
ings of the National Academy of Sciences of the United
States of America 2002;99(26):17089e94.
160. Zhang RL, Zhang ZG, Zhang L, Chopp M. Proliferation and dif-
ferentiation of progenitor cells in the cortex and the subven-
tricular zone in the adult rat after focal cerebral ischemia.
Neuroscience 2001;105(1):33e41.
161. Gierdalski M, Sardi SP, Corfas G, Juliano SL. Endogenous
neuregulin restores radial glia in a (ferret) model of
cortical dysplasia. Journal of Neuroscience 2005;25(37):
8498e504.
162. Gregg C, Weiss S. CNTF/LIF/gp130 receptor complex signaling
maintains a VZ precursor differentiation gradient in the devel-
oping ventral forebrain. Development 2005;132(3):565e78.
163. Nakatomi H, Kuriu T, Okabe S, et al. Regeneration of hippo-
campal pyramidal neurons after ischemic brain injury by re-
cruitment of endogenous neural progenitors. Cell 2002;
110(4):429e41.
164. Gieselmann V, Matzner U, Klein D, et al. Gene therapy: pros-
pects for glycolipid storage diseases. Philosophical Transac-
tions of the Royal of Society London Series B. Biological
Sciences 2003;358(1433):921e5.
165. Givogri MI, Galbiati F, Fasano S, et al. Oligodendroglial progen-
itor cell therapy limits central neurological deficits in mice
with metachromatic leukodystrophy. Journal of Neuroscience
2006;26(12):3109e19.
166. Meng XL, Shen JS, Ohashi T, Maeda H, Kim SU, Eto Y. Brain
transplantation of genetically engineered human neural
stem cells globally corrects brain lesions in the mucopolysac-
charidosis type VII mouse. Journal of Neuroscience Research
2003;74(2):266e77.
167. Svendsen CN, Caldwell MA. Neural stem cells in the develop-
ing central nervous system: implications for cell therapy
through transplantation. [Review] [96 Refs]. Progress in
Brain Research 2000;127:13e34.
272 R. Vawda et al.