Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Stem V Conference Poster
Similar to Stem V Conference Poster (20)
Recently uploaded
Recently uploaded (20)
Stem V Conference Poster
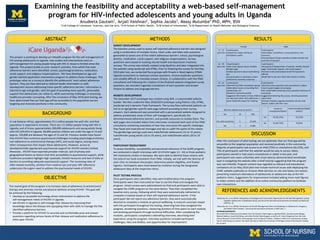
- 1. ABSTRACT BACKGROUND OBJECTIVE METHODS RESULTS DISCUSSION REFERENCES AND ACKNOWLEDGEMENTS Examining the feasibility and acceptability a web-based self-management program for HIV-infected adolescents and young adults in Uganda Anudeeta Gautam1 , Anjali Vaishnav2 , Sophia Jacobs3 , Massy Mutumba4 PhD, MPH, BSN 1 U-M College of Literature, Sciences, and the Arts, 2 U-M School of Public Health, 3 U-M School of Information, 4 U-M Department of Health Behavior and Biological Sciences ACKNOWLEDGEMENTS We would like to thank the consultants from the People in Need Agency Uganda (PINA), Asia Namusoke Mbajja, Robinah Babirye, Suubi Ruth Bulya, and Leilah Richter Nakimbugwe, as well as Dr. Henry Mugerwa from the Joint Clinical Research Centre (JCRC), Namungongo Fund for Special Children, Children’s AIDS Fund, and Kasenyi Landing Site for welcoming our project. We would also like to thank the University of Michigan School of Nursing for funding this project. In sub-Saharan Africa, approximately 23.5 million people live with HIV, and that population is expected to increase. There are 1.5 million people living with HIV in Uganda, and of those, approximately 300,000 adolescents and young adults living with HIV (AYLHIV) in Uganda. 96,000 positive children are under the age of 14 and approx. 150,000 are between the ages of 15 and 24. Previous studies have found that AYLHIV face numerous psychosocial challenges including psychological distress, non-adherence to antiretroviral therapy (ART), and social stigma, among many other consequences that impact these adolescents. However, access to developmentally appropriate psychosocial support for AYLHIV remains limited. Moreover, AYLHIV have reported provider mistrust, lack of privacy and geographical factors as factors that limit accessibility to psychosocial support, while healthcare providers highlight high caseloads, limited resources and lack of skills as barriers to providing adequate psychosocial support. The increasing rates of AIDS-related mortality, attrition from medical care and poor ART adherence underscore the urgent need to address the psychosocial needs of AYLHIV. The overall goal of this program is to increase rates of adherence to antiretroviral therapy and promote mental and physical wellness among AYLHIV. This goal will be achieved by the following: • Develop an accessible technology driven intervention to address the self-management needs of AYLHIV in Uganda. • Aid AYLHIV in Uganda to self-manage their disease by improving their knowledge about the disease and equipping them with skills to manage the five identified adherence barriers. • Provide a platform for AYLHIV to securely and comfortably pose and answer questions regarding various facets of their disease and medication adherence to other peer AYLHIV. After the conclusion of pilot testing, we are optimistic that our final app will be accessible to the targeted population and received positively in the community. Majority of participants had access to an iPad (75%) or smartphone (56.25%), and 75% of participants said that the website would be easy to access. Many participants owned or had used a smartphone or tablet in the past, and participants who were unfamiliar with smart devices demonstrated remarkable ease in navigating the website after a brief tutorial suggesting that the program was user-friendly. Program content was regarded as relevant and educational. Limitations of our May 2019 pilot test include technical issues with deploying the iCARE website publically on Amazon Web-Services on-site and heavy rain season preventing maximum attendance of adolescents at adolescent day at the HIV pediatric clinics. Suggestions for improvement included adding more male figures to video content and the addition of an online community platform to facilitate user-interactions. SURVEY DEVELOPMENT The baseline survey used to assess self-reported adherence barriers was designed using a combination of multiple choice, Likert scale, and table style questions generated to assess one of five salient adherence barriers: school, psychological distress, medication, social support, and religious misperceptions. Survey questions were based on existing mental health and depression inventory surveys. The survey was initially created using Qualtrics and later integrated into the website using JavaScript and HTML. Prior to finalizing the survey for the May 2019 pilot test, we conducted focus groups with People in Need Agency (PINA) Uganda consultants to rephrase unclear questions, remove duplicate questions, and simplify difficult to translate answer choices. In collaboration with the PINA consultants and following the creation of the finalized website-integrated survey questions, we recorded Lugandan translations of each question and answer choices to address any language barriers. WEBSITE DEVELOPMENT The December 2017 prototype was created using WiX, a customizable website builder. We then coded the May 2018/2019 prototype using Python, CSS, HTML, JavaScript and a dynamic Flask framework. The survey flow redirected patients via link to an age/gender-specific web-page tailored according to their survey answers. Each adolescent was presented with a personalized website designed to address problematic areas of their self-management, specifically the aforementioned adherence barriers, and provide resources to resolve them. The web pages also included videos from interviews conducted with each of the PINA consultants containing anecdotes of how they overcame HIV-specific challenges they faced and inspirational messages and tips to uplift the spirits of the viewer. The gender/age pairings used were male/female adolescents (13 to 15 years), male/female young adults (16 to 19 years), and male/female adults (20 to 24 years). PARTICIPANT RECRUITMENT To assess feasibility, acceptability and perceived relevance of the iCARE program, we conducted in depth interviews with 32 AYLHIV (ages 13 - 24) at three pediatric HIV treatments centers in Kampala. We were able to identify these centers with the help of our local consultants from PINA. Initially, we met with the director of each clinic to introduce the project, determine patient eligibility, and finalize logistics. Participants were interviewed by invitation during the designated adolescent days at the respective clinics. PILOT TESTING PROCESS Once participants were identified, they were briefed about the program. Participants were then instructed on how to use the iPads and navigate the program. Initial surveys were administered via iPad and participants were able to navigate the iCARE program on the same device. They then completed the baseline entry survey, following which they were automatically redirected to complete a module based on their self-reported adherence barrier. If the participant did not report any adherence barrier, they were automatically directed to complete a module on general wellbeing. A research associate stayed with the participant throughout the testing, observing how they navigated the program, answering questions, measuring duration of time spent on each module, and assisting participants through technical difficulties. After completing the modules, participants completed a debriefing interview, describing their experience using the program. Interview questions included participant challenges, likes and dislikes, and opportunities for improvement. Female Male 13 - 15 years old 4 participants Enjoyed the videos and found translations useful 4 participants Liked videos, translations, survey questions, and resources One participant found a question unclear and was not sure how to proceed 16 - 19 years old 10 participants Liked visual appeal, layout, healthy lifestyle page Disliked questions about alcohol/drug use One participant in secondary school confused by university resources 3 participants Liked general display/order of website, healthy lifestyle page, relationship support, and social support Worried uneducated people would find questions difficult Would like to see men share their stories in videos 20 - 24 years old 3 participants Liked that the PINA consultants openly talked about issues surrounding their relationships, etc. Wanted to customize profile Suggested information on how children can help each other with adherence, a social media-like aspect for chatting 8 participants Liked the survey questions and consultants in videos Found support pages encouraging Felt comfortable answering survey questions because of anonymity Suggested shortening the survey, removing questions about food Wanted complete Luganda translation of site, chat feature, videos with HIV+ men Was the website easy to access? Yes 24 75% Yes, with assistance 5 15.62% No 3 9.38% Access to smartphone/tablet? Used smartphone/tablet before? Yes 18 (56.25%) 24 (75%) No 14 (43.75%) 8 (25%) This project is working to develop an mHealth program for the self-management of HIV among adolescents in Uganda. Few studies and interventions exist on self-management for young people living with HIV in resource-limited areas like Uganda. This project builds on prior research activities, from which five main adherence barriers were identified: school, psychological distress, medication, social support, and religious misperceptions.. We have developed an age and gender tailored application intervention program to address these challenges. This prototype relies on a survey to identify the adolescents’ most salient adherence barriers. They are then directed to tailored health information or skills development lessons addressing those specific adherence barriers. Information is tailored to age and gender, with the goal of providing more specific, personable support that adolescents can relate to, while overcoming challenges in accessing healthcare provider counseling. After the conclusion of May 2019 pilot testing, we have determined that our final app will be accessible to the population we are targeting and received positively in the community. Mutumba, M., et al. (2018). Perceptions of HIV Self-Management Roles and Challenges in Adolescents, Caregivers, and Health Care Providers. Journal of the Association of Nurses in AIDS Care, 1. Mutumba, M., et al. (2019). Perceptions of Strategies and Intervention Approaches for HIV Self-Management among Ugandan Adolescents: A Qualitative Study, Journal of the International Association of Providers of AIDS Care (JIAPAC), 18.