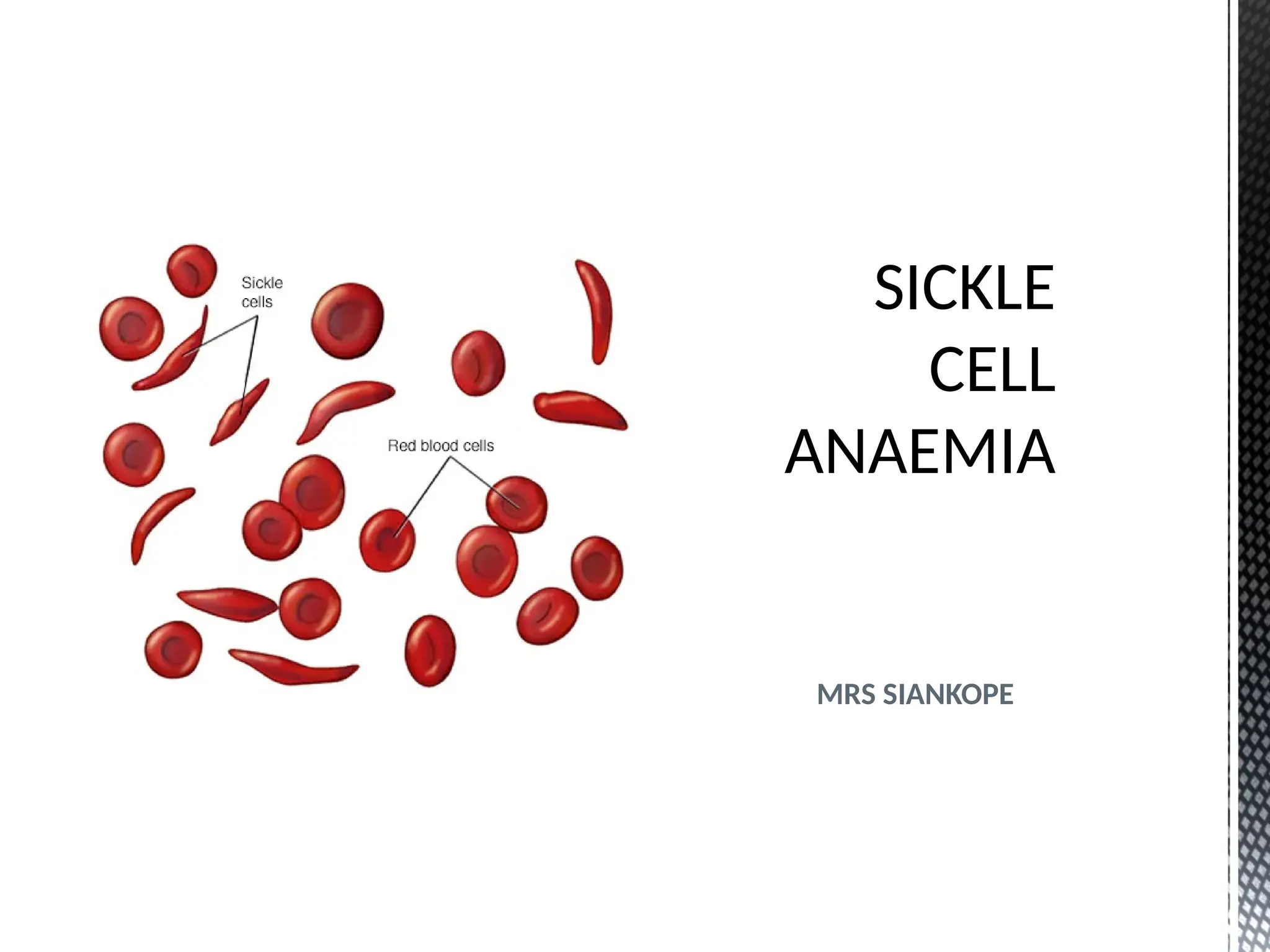
INTRODUCTION
•Sickle cell disease(SCD) is a potentially
devastating condition that is caused by an
autosomal (non sex chromosomal)
recessive inherited hemoglobinopathy
which results in the vaso-occlusive
phenomena and haemolysis.
03/08/2025 2
3.
Intro’
•The severity ofthe complications that
occur with this disorder are widely
variable, but overall mortality is increased
and life expectancy decreased when
compared to the general population.
•Sickle-cell is a hereditary blood disorder
due to the presence of an abnormal
hemoglobin S (HbS).
03/08/2025 3
4.
Intro’
• The sicklingoccurs because of a
mutation in the hemoglobin gene.
• Life expectancy is shortened from 120 to
less than 30 days.
• Sickle-cell disease, usually affect people
(or their descendants) from parts of
tropical and subtropical regions
03/08/2025 4
5.
GENERAL OBJECTIVES:
At theend of the discussion, students
should be able to demonstrate
knowledge and understand Sickle cell
disease and its management.
03/08/2025 5
6.
SPECIFIC OBJECTIVES
At theend of the lesson students should
be able to;
Define sickle cell disease
Outline the types of sickle cell disease.
Explain the pathophysiology of Sickle
cell aneamia
State the signs of symptoms of Sickle
cell aneamia.
03/08/2025 6
7.
SPECIFIC OBJECTIVES CONT’D
Describethe management of Sickle cell
aneamia.
Outline the complications of Sickle cell
aneamia.
State the types of Sickle cell crises
Mention the predisposing factors to
sickling of red blood cell in Sickle cell
aneamia.
03/08/2025 7
8.
SICKLE CELL DISEASE
Itis a severe, chronic, hereditary
haemolytic disorder due to the
homozygous presence of haemoglobin
S, usually characterized by pallor and
recurrent crises. (Baliga2005)
03/08/2025 8
9.
SICKLE CELL DISEASECONT’D
• Sickle cell disease is a severe haemolytic
anaemia occurring in persons who are
homozygous for sickle cell gene,
Characterized by episodes of pain
caused by occlusion of small blood
vessels by sickled red blood cells.
( Lippincott & Wilkins 2001)
03/08/2025 9
10.
TYPES OF SICKLECELL DISEASE
There are basically three, i.e
Sickle cell disease (sickle cell
Anaemia): There is homozygous
inheritance of Hb S (Hb SS). It is
symptomatic.
Sickle cell trait: There is heterozygous
inheritance of Hb S (Hb SA). It is
asymptomatic.
03/08/2025 10
11.
CONT’D
Sickle cell syndromes:Associated with
presence of Hb S (Hb SC sickle cell Hb C)
HBSD (Sickle cell Hb D)
03/08/2025 11
12.
TYPES OF HAEMOGLOBIN
AdultHaemoglobin (HbA) denoted be
the letter A
Composed of 2 alpha and 2 beta
chains
Fetal haemoglobin (HbF) denoted by
the letter F
Composed of 2 alpha and 2 gamma
chains
Other abnormal Hb include: C (Hb C -
lysine substituted for glutamic acid), D
03/08/2025 12
13.
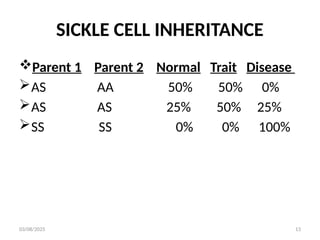
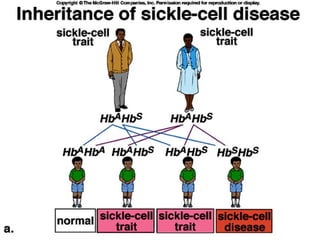
SICKLE CELL INHERITANCE
Parent1 Parent 2 Normal Trait Disease
AS AA 50% 50% 0%
AS AS 25% 50% 25%
SS SS 0% 0% 100%
03/08/2025 13
PATHOPHYSIOLOGY
The Haemoglobin Aconsists of 4
molecules of haem folded in 1 molecule
of globin.
Each globin molecule consists of 2
alpha and 2 beta chains.
The amino acid sequence on the beta
chain is altered at the 6th
position of the
574 amino acids that makes up the
globin fraction of hemoglobin
(Lippincott & Wilkins, 2001).
03/08/2025 16
17.
• The hydrophilicamino acid glutamine is
replaced by the hydrophobic amino acid
valine changing the properties of the
Hemoglobin.
03/08/2025 17
18.
The gene defectis a known mutation of
a single nucleotide of the β-globin gene,
which results in glutamic acid being
substituted by valine at position 6.
Haemoglobin S with this mutation is
referred to as HbS, as opposed to the
normal adult HbA.
The genetic disorder is due to the
mutation of a single nucleotide, from a
GAG to GTG codon mutation.
03/08/2025 18
19.
This change resultsin change of
characteristics of the haemoglobin.
When the HbS is subjected to low
oxygen tension the abnormal beta
chain contracts and piles together
within the red blood cell this distorts
the shape of the red blood cell.
03/08/2025 19
20.
• The cellsunder go polymerization and
clump together and form masses of
RBCs called tactoids. This distorts the
cell structure of the red blood cell.
• Usually the cell returns their normal
shape, after the low oxygen conditions
are removed and proper oxygenation
occurs.
03/08/2025 20
21.
Although the cellmay appear normal at
least some of the Hb remains twisted
decreasing the flexibility of the cell.
The repeated sickling of the cell lead to
permanent distortion of the cell
structure adopting a characteristic
crescent (sickled) shape due to cell
membrane damage.
03/08/2025 21
22.
The sickled cellincreases the viscosity
of blood and the cells easily attach to
the endothelial cell causing occlusion of
the red blood cell. These cells block the
blood flow leading to sickling of other
RBCs with more obstruction of blood
vessels and ischemia of the affected
tissues.
03/08/2025 22
23.
• Repeated episodesof ischaemia leads
to progressive damage from infarction
of the affected tissues
The cell also becomes more fragile and
easily hemolysed due to structural
change. Its life span reduces from 120
to less than 30 days.
The reduced life span of the RBC and
increased destruction of red blood cells
causes haemolytic anaemia.
03/08/2025 23
24.
• The patientalso experiences periodic
episodes of cellular sickling called
crises, characterized by high fever,
general body pain
03/08/2025 24
25.
SIGNS AND SYMPTOMSOF SICKLE
CELL DISEASE
Attacks of abdominal pain due to tissue
ischaemia
Bone pain due to ischaemia
Breathlessness due to cardio pulmonary
involvement and intra pulmonary sickling
Delayed growth and puberty because
energy demands of the bone marrow for
red blood cell production compete with
the demands of a growing body.
Fatigue due to tissue hypoxia
03/08/2025 25
26.
Fever due theinflammatory reaction
caused by tissue infarction and sometimes
co-existing infections
Jaundice due to increased levels of
bilirubin as a result of increased
haemolysis
Pallor due to low hemoglobin
Tachycardia as the heart attempts to
compensate for hypoxia
Susceptibility to infections due to low
immunity
03/08/2025 26
27.
Bloody urine (haematuria)due to renal
damage following repeated tissue infarction
Chest pain due to pulmonary infarction or
cardiac ischemia
Restlessness especially during crises due to
pain
Painful erection (priapism; this occurs in 10
- 40% of sufferers of the disease) due to
blood being trapped by occluded blood
vessel
03/08/2025 27
28.
TYPES OF CRISES
Thereare four (4) types of sickle cell
crises ie;
Vaso-occlusive crisis
Aplastic crisis
Sequestration crisis
Haemolytic crisis.
03/08/2025 28
29.
VASO-OCCLUSIVE CRISIS
The vaso-occlusivecrisis is caused by
sickle-shaped red blood cells that
obstruct capillaries causing ischaemia
and infarction.
This results in ischaemia, pain, necrosis
and often organ damage.
The frequency, severity, and duration
of these crises vary considerably.
03/08/2025 29
30.
• Painful crisesare treated with
hydration, analgesics, and blood
transfusion; pain management requires
opioid administration at regular
intervals until the crisis has settled.
• For milder crises, a subgroup of
patients manage on NSAIDs (such as
diclofenac or naproxen).
03/08/2025 30
31.
SPLENIC SEQUESTRATION CRISIS
Splenic sequestration crises: are acute,
painful enlargements of the spleen.
The sinusoids and gates would open at
the same time resulting in sudden
pooling of the blood into the spleen and
circulatory defect leading to sudden
hypovolaemia.
The abdomen becomes bloated and
very hard. Splenic sequestration crises
are considered an emergency.
03/08/2025 31
32.
If not treated,patients may die within
1–2 hours due to circulatory failure. It is
the commonest cause of death in
children with sickle cell.
Management is supportive, sometimes
with blood transfusion. This crises is
transient, it continues for 3–4 hours and
may last for one day.
03/08/2025 32
33.
Because of itsnarrow vessels and function in
clearing defective red blood cells, the spleen
is frequently affected.
It is usually infarcted before the end of
childhood in individuals suffering from sickle-
cell anaemia.
This autosplenectomy increases the risk of
infection from encapsulated organisms (such
as Haemophilus influenza and streptococcus
pneumoniae), therefore, preventive
antibiotics and vaccinations are
recommended.
03/08/2025 33
34.
APLASTIC CRISIS
Aplastic crisesoccur when there is acute
worsening of the patient's baseline
anaemia.
This crisis is triggered by parvovirus B19,
which directly affects erythropoiesis by
invading the red cell precursors and
multiplying in them and destroying them.
Parvovirus infection nearly completely
prevents red blood cell production.
03/08/2025 34
35.
In normal individuals,this is of little
consequence, but the shortened red
cell life of sickle-cell patients’ results in
an abrupt, life-threatening situation.
Reticulocyte counts drop dramatically
during the disease (causing
reticulocytopenia),
This leads to low oxygen tension
precipitating a crisis
03/08/2025 35
36.
HAEMOLYTIC CRISIS
The HbSis very fragile leading to a high
red blood cells break down.
This leads to acute accelerated drops in
haemoglobin level.
The result is low oxygen tension there
by precipitating a crisis.
Management is supportive, sometimes
with blood transfusions
03/08/2025 36
37.
PREDISPOSING FACTORS TOA CRISIS
Dehydration
Infection
Strenuous exercises
Severe trauma
Exposure to cold
Change of altitude from low to high
with low oxygen concentration
03/08/2025 37
38.
MANAGEMENT OF APATIENT WITH
SICKLE CELL ANAEMIA
HEALTH HISTORY
When taking specific history of sickle
cell from the caretaker, ask questions
that are more specific to the condition.
03/08/2025 38
39.
CONT’D
PHYSICAL EXAMINATION
Physical examinationincludes: -
Direct observation / inspection of the
entire body to rule out the clinical
features of sickle cell eg. Anaemia,
growth retardation,etc
03/08/2025 39
40.
CONT’D
INVESTIGATIONS
Full blood countwill reveal haemoglobin
levels in the range of 6–8 g/dL with a high
Reticulocyte count (as the bone marrow
compensates for the destruction of sickle
cells by producing more red blood cells).
Sickling test will show sickling of cells
(This test does not tell you if patient is
trait or disease)
03/08/2025 40
41.
TREATMENT
Antibiotics e.g. e.g.crystalline penicillin
1-2mu qid for 5/7
Oxygen therapy to relieve hypoxemia
e.g. 5l/minute
Narcotic analgesics like pethidine
1mg/kg body weight for 3/7 or
morphine
Folic acid 5-10 mg od for 14/7
Blood transfusion with packed cell may
be give
03/08/2025 41
42.
TREATMENT CONT’D
If malariais present antimalarials will be
given
Non steroidal anti inflammatory drugs
such as aspirin 150-600mg tds for 3/7 or
diclofenac or Brustan.
Iv fluid with normal saline to relieve
dehydration e.g. 150ml /kg in 24hours
03/08/2025 42
CONT’D
Nursing intervention/ rationale
Iwill:-
Offer prescribed pethidine 1mg/kg
body weight PRN in order to relieve pain
and comfort
I will do warm compresses on the
painful areas to relieve pain
I will give prescribed normal saline to
rehydrate patient thereby relieve
ischaemia and subsequently pain
03/08/2025 44
CONT’D
Problem/needs identified
Ineffective breathingpattern
Nursing diagnosis
Ineffective breathing pattern due to
intrapulmonary sickling resulting in impaired
gaseous exchange manifested by use of
accessory muscles of respiration and flaring of
nares
Objective
To relieve improve breathing pattern within
30 minutes
03/08/2025 46
47.
CONT’D
Nursing interventions/ rationale
Iwill offer oxygen therapy 2-3l/minute
If patient is old enough I will prop him
up to promote lung expansion and
thereby relieving dyspnea
Expected outcome
Breathing pattern improved within 30
minutes evidenced by reduced use of
accessory muscles and no flaring of
nares
03/08/2025 47
48.
Other problems
• Activityintolerance due to pain
• Anxiety due to repeated crises
• Knowledge deficit if older child
• Impaired tissue oxygen perfusion
• Risk for infection
• Risk for cerebral tissue damage
03/08/2025 48
49.
POSSIBLE COMPLICATIONS
Sickle-cellanaemia can lead to various
complications, including:
Post Auto splenectomy infection (OPSI),
this is due to functional asplenia
(absence of spleen function), caused by
encapsulated organisms such as
Streptococcus pneumoniae and
Haemophilus influenzae..
Priapism due to trapping of blood in the
penis
03/08/2025 49
50.
CONT’D
Stroke, which canresult from a
progressive narrowing of blood vessels,
preventing oxygen from reaching the
brain. Cerebral infarction occurs in
children.
Cholelithiasis (gallstones) and
cholecystitis, which may result from
excessive bilirubin production and
precipitation due to prolonged
haemolysis
03/08/2025 50
51.
CONT’D
Avascular necrosis (asepticbone
necrosis) of the hip and other major
joints, which may occur as a result of
ischaemia.
Decreased immune reactions due to
hyposplenism (malfunctioning of the
spleen).
03/08/2025 51
52.
CONT’D
Acute papillary necrosisin the kidneys.
Chronic renal failure due to Sickle cell
nephropathy
Leg ulcers due to ischaemia.
In eyes, background retinopathy,
proliferative retinopathy, vitreous
haemorrhages and retinal
detachments, resulting in blindness.
03/08/2025 52
53.
CONT’D
During pregnancy (inadolescence stage)
intrauterine growth retardation,
spontaneous abortion, and pre-eclampsia.
Cardiomyoparthies due to pulmonary
hypertension leading to strain on the right
ventricle and a risk of heart failure. Typical
symptoms are shortness of breath,
decreased exercise tolerance and
episodes of syncope.
03/08/2025 53
54.
PREVENTING CRISES
The followingsteps can help prevent a sickle cell crisis:
Maintain good oxygen levels and prevent
dehydration.
Avoid strenuous activities, stress, smoking, high-
altitudes, no pressurized flights, and other events
that reduce your oxygen level.
Always have plenty of fluids with you
Avoid too much sun exposure
Consider having the child with sickle cell anemia
wear a Medic Alert bracelet. Share the above
information with teachers and other caretakers,
when necessary.
03/08/2025 54
55.
REFERRENCES
Lewis S.M., ColierI. C. and Heitkemper,
M.M. (1996) Medical and Surgical
Nursing: Assessment and Management
of clinical practice, 4th
edition, Mosby –
Year Book Inc, st Louis.
Marlow D. (1973) Text book of
Paediatric Nursing, 4th
edition,
Saunders comp, Philadelphia.
03/08/2025 55
56.
Smeltzer S.C. &Bare B.G.(2004), Text book of
Medical and Surgical Nursing, 10th
edition,
Lippincott Willam & Wilkins, Philadelphia.
Wong L. D. (1995), Nursing care of Infants
and Children. 5th
edition, Mosby Year Book
inc. st Louis, USA.
Roper N., Logan W.W. & Tierney A.J. (1980).
The Elements of Nursing. Churchill
Livingstone
03/08/2025 56