Scrub typhus is an acute infectious illness caused by the bacteria Orientia tsutsugamushi, which is transmitted to humans through bites from trombiculid mites. It is endemic in parts of Asia and the Pacific. Symptoms include high fever, headache, rash and eschar at the site of the mite bite. Diagnosis is made through serologic tests detecting antibodies or PCR. Treatment is with doxycycline or azithromycin. Preventive measures include protective clothing, insect repellents and vector control. With treatment, prognosis is good, but mortality can be high without treatment or if complications develop.
Neglected tropical diseases nt ds-kananura-egesa-finalKananura Keneth
We give a highlight of common neglected tropical diseases in Uganda and East Africa region.
Compiled by me (Dr.Keneth Kananura, MBChB,Mak) and my supervisor, Dr. Moses Egesa, PhD-MRC-Uganda)
It is a type of Infectious disease caused by the Rickettsia genus of bacteria.
Rickettsiae are a heterogeneous group of small, obligately intracellular, gram-negative coccobacilli and short bacilli, most of which are transmitted by a tick, mite, flea, or louse vector.
Except in the case of louse-borne typhus, humans are incidental hosts.
Neglected tropical diseases nt ds-kananura-egesa-finalKananura Keneth
We give a highlight of common neglected tropical diseases in Uganda and East Africa region.
Compiled by me (Dr.Keneth Kananura, MBChB,Mak) and my supervisor, Dr. Moses Egesa, PhD-MRC-Uganda)
It is a type of Infectious disease caused by the Rickettsia genus of bacteria.
Rickettsiae are a heterogeneous group of small, obligately intracellular, gram-negative coccobacilli and short bacilli, most of which are transmitted by a tick, mite, flea, or louse vector.
Except in the case of louse-borne typhus, humans are incidental hosts.
CHAPTER 1 SEMESTER V PREVENTIVE-PEDIATRICS.pdfSachin Sharma
This content provides an overview of preventive pediatrics. It defines preventive pediatrics as preventing disease and promoting children's physical, mental, and social well-being to achieve positive health. It discusses antenatal, postnatal, and social preventive pediatrics. It also covers various child health programs like immunization, breastfeeding, ICDS, and the roles of organizations like WHO, UNICEF, and nurses in preventive pediatrics.
Telehealth Psychology Building Trust with Clients.pptxThe Harvest Clinic
Telehealth psychology is a digital approach that offers psychological services and mental health care to clients remotely, using technologies like video conferencing, phone calls, text messaging, and mobile apps for communication.
CHAPTER 1 SEMESTER V PREVENTIVE-PEDIATRICS.pdfSachin Sharma
This content provides an overview of preventive pediatrics. It defines preventive pediatrics as preventing disease and promoting children's physical, mental, and social well-being to achieve positive health. It discusses antenatal, postnatal, and social preventive pediatrics. It also covers various child health programs like immunization, breastfeeding, ICDS, and the roles of organizations like WHO, UNICEF, and nurses in preventive pediatrics.
Telehealth Psychology Building Trust with Clients.pptxThe Harvest Clinic
Telehealth psychology is a digital approach that offers psychological services and mental health care to clients remotely, using technologies like video conferencing, phone calls, text messaging, and mobile apps for communication.
Struggling with intense fears that disrupt your life? At Renew Life Hypnosis, we offer specialized hypnosis to overcome fear. Phobias are exaggerated fears, often stemming from past traumas or learned behaviors. Hypnotherapy addresses these deep-seated fears by accessing the subconscious mind, helping you change your reactions to phobic triggers. Our expert therapists guide you into a state of deep relaxation, allowing you to transform your responses and reduce anxiety. Experience increased confidence and freedom from phobias with our personalized approach. Ready to live a fear-free life? Visit us at Renew Life Hypnosis..
Antibiotic Stewardship by Anushri Srivastava.pptxAnushriSrivastav
Stewardship is the act of taking good care of something.
Antimicrobial stewardship is a coordinated program that promotes the appropriate use of antimicrobials (including antibiotics), improves patient outcomes, reduces microbial resistance, and decreases the spread of infections caused by multidrug-resistant organisms.
WHO launched the Global Antimicrobial Resistance and Use Surveillance System (GLASS) in 2015 to fill knowledge gaps and inform strategies at all levels.
ACCORDING TO apic.org,
Antimicrobial stewardship is a coordinated program that promotes the appropriate use of antimicrobials (including antibiotics), improves patient outcomes, reduces microbial resistance, and decreases the spread of infections caused by multidrug-resistant organisms.
ACCORDING TO pewtrusts.org,
Antibiotic stewardship refers to efforts in doctors’ offices, hospitals, long term care facilities, and other health care settings to ensure that antibiotics are used only when necessary and appropriate
According to WHO,
Antimicrobial stewardship is a systematic approach to educate and support health care professionals to follow evidence-based guidelines for prescribing and administering antimicrobials
In 1996, John McGowan and Dale Gerding first applied the term antimicrobial stewardship, where they suggested a causal association between antimicrobial agent use and resistance. They also focused on the urgency of large-scale controlled trials of antimicrobial-use regulation employing sophisticated epidemiologic methods, molecular typing, and precise resistance mechanism analysis.
Antimicrobial Stewardship(AMS) refers to the optimal selection, dosing, and duration of antimicrobial treatment resulting in the best clinical outcome with minimal side effects to the patients and minimal impact on subsequent resistance.
According to the 2019 report, in the US, more than 2.8 million antibiotic-resistant infections occur each year, and more than 35000 people die. In addition to this, it also mentioned that 223,900 cases of Clostridoides difficile occurred in 2017, of which 12800 people died. The report did not include viruses or parasites
VISION
Being proactive
Supporting optimal animal and human health
Exploring ways to reduce overall use of antimicrobials
Using the drugs that prevent and treat disease by killing microscopic organisms in a responsible way
GOAL
to prevent the generation and spread of antimicrobial resistance (AMR). Doing so will preserve the effectiveness of these drugs in animals and humans for years to come.
being to preserve human and animal health and the effectiveness of antimicrobial medications.
to implement a multidisciplinary approach in assembling a stewardship team to include an infectious disease physician, a clinical pharmacist with infectious diseases training, infection preventionist, and a close collaboration with the staff in the clinical microbiology laboratory
to prevent antimicrobial overuse, misuse and abuse.
to minimize the developme
Welcome to Secret Tantric, London’s finest VIP Massage agency. Since we first opened our doors, we have provided the ultimate erotic massage experience to innumerable clients, each one searching for the very best sensual massage in London. We come by this reputation honestly with a dynamic team of the city’s most beautiful masseuses.
Leading the Way in Nephrology: Dr. David Greene's Work with Stem Cells for Ki...Dr. David Greene Arizona
As we watch Dr. Greene's continued efforts and research in Arizona, it's clear that stem cell therapy holds a promising key to unlocking new doors in the treatment of kidney disease. With each study and trial, we step closer to a world where kidney disease is no longer a life sentence but a treatable condition, thanks to pioneers like Dr. David Greene.
CRISPR-Cas9, a revolutionary gene-editing tool, holds immense potential to reshape medicine, agriculture, and our understanding of life. But like any powerful tool, it comes with ethical considerations.
Unveiling CRISPR: This naturally occurring bacterial defense system (crRNA & Cas9 protein) fights viruses. Scientists repurposed it for precise gene editing (correction, deletion, insertion) by targeting specific DNA sequences.
The Promise: CRISPR offers exciting possibilities:
Gene Therapy: Correcting genetic diseases like cystic fibrosis.
Agriculture: Engineering crops resistant to pests and harsh environments.
Research: Studying gene function to unlock new knowledge.
The Peril: Ethical concerns demand attention:
Off-target Effects: Unintended DNA edits can have unforeseen consequences.
Eugenics: Misusing CRISPR for designer babies raises social and ethical questions.
Equity: High costs could limit access to this potentially life-saving technology.
The Path Forward: Responsible development is crucial:
International Collaboration: Clear guidelines are needed for research and human trials.
Public Education: Open discussions ensure informed decisions about CRISPR.
Prioritize Safety and Ethics: Safety and ethical principles must be paramount.
CRISPR offers a powerful tool for a better future, but responsible development and addressing ethical concerns are essential. By prioritizing safety, fostering open dialogue, and ensuring equitable access, we can harness CRISPR's power for the benefit of all. (2998 characters)
R3 Stem Cells and Kidney Repair A New Horizon in Nephrology.pptxR3 Stem Cell
R3 Stem Cells and Kidney Repair: A New Horizon in Nephrology" explores groundbreaking advancements in the use of R3 stem cells for kidney disease treatment. This insightful piece delves into the potential of these cells to regenerate damaged kidney tissue, offering new hope for patients and reshaping the future of nephrology.
QA Paediatric dentistry department, Hospital Melaka 2020Azreen Aj
QA study - To improve the 6th monthly recall rate post-comprehensive dental treatment under general anaesthesia in paediatric dentistry department, Hospital Melaka
Medical Technology Tackles New Health Care Demand - Research Report - March 2...pchutichetpong
M Capital Group (“MCG”) predicts that with, against, despite, and even without the global pandemic, the medical technology (MedTech) industry shows signs of continuous healthy growth, driven by smaller, faster, and cheaper devices, growing demand for home-based applications, technological innovation, strategic acquisitions, investments, and SPAC listings. MCG predicts that this should reflects itself in annual growth of over 6%, well beyond 2028.
According to Chris Mouchabhani, Managing Partner at M Capital Group, “Despite all economic scenarios that one may consider, beyond overall economic shocks, medical technology should remain one of the most promising and robust sectors over the short to medium term and well beyond 2028.”
There is a movement towards home-based care for the elderly, next generation scanning and MRI devices, wearable technology, artificial intelligence incorporation, and online connectivity. Experts also see a focus on predictive, preventive, personalized, participatory, and precision medicine, with rising levels of integration of home care and technological innovation.
The average cost of treatment has been rising across the board, creating additional financial burdens to governments, healthcare providers and insurance companies. According to MCG, cost-per-inpatient-stay in the United States alone rose on average annually by over 13% between 2014 to 2021, leading MedTech to focus research efforts on optimized medical equipment at lower price points, whilst emphasizing portability and ease of use. Namely, 46% of the 1,008 medical technology companies in the 2021 MedTech Innovator (“MTI”) database are focusing on prevention, wellness, detection, or diagnosis, signaling a clear push for preventive care to also tackle costs.
In addition, there has also been a lasting impact on consumer and medical demand for home care, supported by the pandemic. Lockdowns, closure of care facilities, and healthcare systems subjected to capacity pressure, accelerated demand away from traditional inpatient care. Now, outpatient care solutions are driving industry production, with nearly 70% of recent diagnostics start-up companies producing products in areas such as ambulatory clinics, at-home care, and self-administered diagnostics.
2. DEFINITION
Scrub typhus is an acute, febrile,
infectious illness that is caused by
Orientia tsutsugamushi
(an obligate (absolute/compel)
Intracellular gram-negative bacteria).
3. Scrub means low shrub & grasses that
harbors the vector (trombiculid mites
also called chiggers).
However, this term is not entirely accurate, in
that scrub typhus can also be prevalent in
areas such as sandy beaches, mountain,
deserts and rain forests.
5. HISTORY OF DISEASES:-
Scrub typhus is one of the tropical rickettsial
diseases.
This was first described in China in 313 AD.
Bacteria was first isolated in Japan in 1930 AD.
Orientia is genus of bacteria in family Rickettsiaceae.
US cases have been imported from regions of the
“tsutsugamushi triangle,” which extends from
northern Japan and eastern Russia in the north to
northern Australia in the south and to Pakistan and
Afghanistan in the west, where the disease is
endemic.
6.
7. Western medicine became especially interested in
scrub typhus during military campaigns fought in
East Asia. During World War II, 18,000 cases were
observed in Allied/suppoter troops stationed in rural
or jungle areas of the Pacific theatre. Scrub typhus
was the second or third most common infection
reported in US troops stationed in Vietnam and still
infects troops in the region.
Currently, it is estimated that about 1 million cases
of scrub typhus occur annually and that as many as
1 billion people living in endemic areas may
have been infected by O.tsutsugamushi at some
time.
8. EPIDEMIOLOGY:-
Scrub typhus is endemic in regions of eastern Asia
and the southwestern Pacific (Korea to Australia)
and from Japan to India and Pakistan.
It is generally a disease of rural villages and
suburban areas and is normally not encountered
in the cities.
Age-, sex-, and race-related demographics
People of all ages are affected equally by scrub
typhus. Men and women are affected with equal
frequency. No race-related differences in incidence
have been documented.
9. IN NEPAL
Aug 2015 after 3 months of Earthquake, case noted
in:- Chitwan, Lalitpur, Dhading,
Sankhuwasabha, Bhojpur, Dhankuta, Siraha,
Kailali & Ramechap.
A total of 101 confirmed scrub typhus cases
were reported from 16 districts in 2015. Out of
them, eight cases died, accounting for a crude
case fatality rate of 8%.
By the end of August 2016, more than 500
confirmed cases and six additional deaths were
reported from the various districts of the
country.
2016—831 cases of scrub typhus were reported in 47
districts and 14 people died by the end of that year.
10. From 2015 to 2017,
1239 scrub typhus cases were
confirmed with the largest outbreak
occurring in 2016 with 831 (67.1%)
cases.
The case fatality rate was 5.7% in 2015
which declined to 1.1% in 2017.
A nationwide outbreak of scrub typhus
was declared as the cases were
detected in 52 out of the 75 districts of
Nepal.
Seasonal trend was observed with a
peak during August and September.
11. a total of 1,999 people were
infected with the disease; in
2020,
In 2021, the number declined
to 1,026.
Over 260 people have been infected
with the disease since the start of
2022 till May 12, 2022.
13. ETIOLOGY
Scrub typhus is caused by Orientia
tsutsugamushi, an obligate intracellular gram-
negative bacterium that lives primarily in mites
Trombicula genus
Leptotrombidium(genus) akamushi(Sp)
Leptotrombidium deliense .
This organism is found throughout the mite’s body but is
present in the greatest number in the salivary
glands.
16. MODE OF TRANSMISSION:-
Scrub typhus is often acquired during occupational
or agricultural exposures because active rice fields
are an important reservoir for transmission.
Taking a rest directly on the grass,
working in short sleeves,
working with bare hands, and
squatting to defecate or urinate posed the highest
risks.
17.
18. Pathophysiology:-
When the mite feeds on rodents (eg, rats,
moles/छुचुन्द्रो, and field mice, which are the
secondary reservoirs for bacteria) or humans,
the parasites are transmitted to the host.
Wild rats serve as the natural reservoir for the chiggers
(and represent a risk factor for human infection), but they
are rarely infected with O tsutsugamushi.
Only larval Leptotrombidium mites (chiggers) transmit the
disease.
Orientia is also transmitted transovarially in mites and can
unbalance the sex ratio of offspring in favor of females, further
propagating infection.
19.
20.
21.
22.
23.
24. SIGNS AND SYMPTOMS
History:
Travelling to scrub typhus endemic area.
Chigger bite (often painless and unnoticed)
Incubation period of 6-20 days (average, 10 days)
25. SYMPTOMS:-
High fever (40-40.5°C [104-105°F]), occurring
more than 98% of the time,
Headaches,
Shaking chills,
Red eye,
Anorexia, abdominal pain, nausea, vomitting
General apathy, regional lymphadenopathy
Cough, difficulty in breathing
Centrifugal (center to periphery) macular rash on
the trunk. In adults, the eschar is often truncal,
whereas children may have lesions in the
perineum.
26.
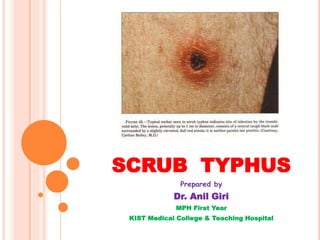
27. Rash; a small, painless, gradually enlarging papule, which
leads to an area of central necrosis and is followed by
eschar formation in centrifugal (central to peripheral)
pattern.
28.
29.
30. PHYSICAL FINDINGS:-
Tender regional or generalized lymphadenopathy,
occurring in 40-97% of cases
Enlargement of the spleen,
Altered consciousness.
If acute hearing loss is present (as may be the case
in as many as one third of patients, according to
some reports), it strongly points toward scrub
typhus.
31.
32. COMPLICATIONS:-
Central nervous system (encephalitis), pulmonary
(ARDS) or cardiac involvement.
Rarely, acute renal failure, shock and disseminated
intravascular coagulation (DIC) .
If the patient does not receive treatment, symptoms
may last for more than 2 weeks; with treatment, the
patient recovers within 36 hours.
33.
34. DIAGNOSIS
Laboratory studies in patients with scrub typhus
may reveal the following:
Early lymphopenia with late lymphocytosis
Decreased CD4:CD8 lymphocyte ratio
Thrombocytopenia
Elevated transaminase (SGOT, SGPT) levels (75-
95% of patients)
Chest radiography may reveal pneumonitis,
especially in the lower lung fields.
35. Laboratory studies of choice are serologic
tests for antibodies, including the
following:
Indirect immunoperoxidase test
Indirect fluorescent antibody test
Dot immunoassay
Rapid immunochromatographic tests for detection
of IgM and IgG
Polymerase chain reaction (PCR) assay
Rapid diagnostic reagent for scrub typhus
Weil-Felix OX-K strain agglutination reaction
38. MANAGEMENT:-
Antibiotic therapy.
Drug of choice:-
Capsule Doxycycline (Tetracycline) 100mg twice
daily for 7-10 days. Provided free by Nepal
government.
For Pregnant & Children:-
Tablet or Syrup Azithromycin (Macrolides) 10mg per
kg per day for 5 days.
Others:-
Rifampicin 600-900mg per day for 7 days.
Clarithromycin 500mg per day for 10 days.
Ciprofloxacin 500mg twice daily for 10days.
39.
40. SUPPORTIVE TREATMENT:-
Normal diet & rest.
Inpatient care may be necessary for patients with
severe scrub typhus. In such cases, meticulous
supportive management is necessary to abort
progression to DIC or circulatory collapse.
41. PREVENTIVE MEASURES
in endemic areas include the following:
Protective clothing:- Wearing a long-sleeved
shirt while working, keeping work clothes off the
grass, and always using a mat to rest outdoors
showed protective associations.
Insect repellents
Short-term vector reduction using
environmental insecticides and vegetation
control.
42.
43. CHEMOPROPHYLAXIS REGIMENS:-
A single dose of doxycycline given weekly, started
before exposure and continued for 6 weeks after
exposure.
No effective vaccine is available.
44. PROGNOSIS:-
Prognosis varies and depends on the
severity of illness, which relates to the
different strains of O tsutsugamushi,
as well as to host factors.
In patients who are not treated,
mortality ranges from 1% to 60%,
depending on the patient’s age, the
geographic area, and the particular
strain responsible for the infection.
45. With appropriate antibiotic treatment,
mortality from scrub typhus is quite rare,
and the recovery period is short and usually
without complications.
However, mortality is still approximately
15% in some areas as a consequence of
missed or delayed diagnosis.[31] If severe
complications such as acute respiratory
distress syndrome (ARDS) arise, mortality
may still be high.