2
Schizophrenia spectrum disorders
•Group of psychiatric diagnoses that share
several clinical features,
• Typically involving reality distortion
• Each is considered a disorder, diagnosed with
a distinct set of diagnostic criteria
• Spectrum conveys the idea that they are
somehow similar to each other
• Tension of distinctiveness and similarity
3.
3
• In the19th century, one view was that all serious mental
disorders were expressions of a single entity, termed by
Griesinger as “Einheitpsychose”, i.e. unitary psychosis.
• Mental disorders could be separated & classified -
Benedict Morel
• Coined the term “demence precoce” for describing a
chronic deteriorative disorder, starting at adolescent &
leading first to withdrawal, odd mannerisms and self
neglect & eventually leading to intellectual deterioration
4.
4
• Emil Kraepelintranslated Morel’s “demence
precoce” into “dementia praecox”, to
emphasize the distinct cognitive decline
(dementia) & early onset (praecox) of the
disorder.
• Eugen Bleuler coined the term
“schizophrenia” in 1911 to mean “splitting” of
the psychic functions. Bleuler made a
distinction between the fundamental &
accessory symptoms of schizophrenia.
5.
5
• Karl Kleist,looked for association between
brain pathology & different subtypes of
psychotic illness
• The term ‘Schizo-Affective Psychosis’ was
first coined by Jacob Kasanin in 1933
• , Kasanin himself believed ‘Schizo-Affective
Psychosis’ to be a subtype of schizophrenia
6.
6
• Evolving viewis the idea that schizophrenia
may represent a point—or end point—on a
continuum of deficit rather than a discrete
disease entity
• Use of epidemiological, genetic and other
family study paradigms for ICD – 10 and DSM
IV
7.
7
SPECTRUM
• Strongest evidence- schizoaffective disorder
and schizotypal personality disorder
• Moderate evidence - paranoid and schizoid
personality disorder
• Recently proposed – research criteria for
another syndrome, called schizotaxia,
8.
8
THEORETICAL ISSUES
• Nowidely accepted rules for determining whether a
syndrome warrants inclusion
• Two traditional lines of evidence –
clinical similarity to schizophrenia
aggregatation in families affected by schizophrenia
(evidence of both the genetic and nongenetic
etiological similarities of the disorder to schizophrenia)
(kendler et al 1985 , seivel et al 1990)
9.
9
SCHIZOAFFECTIVE DISORDER
NOSOLOGY
• DSMII – as a subtype of schizophrenia
DSM III - under “ psychotic disorders not elsewhere classified.”
DSM III R - it became more well defined
DSM IV TR- incorporated the time frame of 1 month
duration of schizophrenic symptoms
• ICD 9 – like DSM II
ICD 10- Schizoaffective disorder applied to patients who
have co-occuring mood symptoms and
schizophrenic symptoms
10.
10
EPIDEMIOLOGY
The life timeprevalence of schizoaffective
disorder is
< 1 %( .5 -.8 %)
Depressive subtype – older > younger
Bipolar subtype - young > old
Female > Male
Age of onset of female later than male
11.
11
DIAGNOSIS AND CLINICALFEATURES
DSM IV TR
A) uninterrupted period of illness in which sometime there has
been an affective episode concurrent with symptoms of criteria
A of schizophrenia.
B) during same episode, delusions and hallucinations must be
present for atleast 2 weeks in the absence of
mood symptoms.
C) symptoms of mood episode is present for substantial
portion of active symptoms & residual symptoms.
D) it is not due to substance / general medical condition
SPECIFIER- Bipolar/Depressive type
12.
12
Clinical Similarities toSchizophrenia
• Schizoaffective Disorder
diagnosis of schizoaffective disorder, which
specify that Criterion A of schizophrenia must
be satisfied and that delusions or
hallucinations must be present
depressive type is believed to lie nearer the
schizophrenia spectrum
bipolar type is believed to that of traditional
mood disorders
13.
13
Schizotypal Personality Disorder
•diagnosis based on the presence of both social and
cognitive deficits
• reflect those of schizophrenia but with less severity
• ideas of reference, odd beliefs, magical thinking, unusual
perceptual experiences, and suspiciousness
• odd thinking, speech, and behavior - disorganized type
schizophrenia
• appearance of affective disturbance, the lack of close
friends, and the excessive social anxiety resembles social
dysfunction of schizophrenia (i.e., negative symptoms).
14.
14
Paranoid Personality Disorder
•characterized by a pervasive distrust and
suspiciousness of other
• Though shares only this single group of
symptoms with schizophrenia,features are
central to the diagnosis of paranoid type
schizophrenia;
15.
15
Schizoid Personality Disorder
•Principal clinical feature - social dysfunction,
ranging from aversion of social relationships to
restricted affective expression in interpersonal
settings
• Symptoms similar to the social dysfunction
that is a fundamental feature of schizophrenia
but less pronounced
16.
16
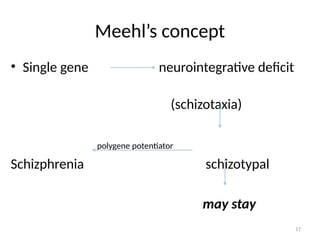
Schizotaxia
• Not describedin the DSM-IV-TR
• Originally formulated by Paul Meehl in 1962
• Represented the genetic predisposition to
schizophrenia that led, almost invariably, to
either schizotypy or schizophrenia, depending on
environmental circumstances
• Reformulated only recently as a meaningful
clinical syndrome as well as a relatively specific
reflection of the vulnerability to schizophrenia
18
Schizotaxia - currentconcept
• (1) As a result of the interaction between a
genetic predisposition and the biological
consequences of early adverse environmental
experiences (e.g., pregnancy complications)
• (2) includes meaningful, definable clinical and
neuropsychological symptoms;
• (3) remains a stable syndrome in many individuals;
• (4) is similar conceptually and phenomenally to
negative schizotypal personality disorder
19.
19
Familial Aggregation withSchizophrenia
• Schizoaffective Disorder
More than a dozen family studies , twin
studies , and adoption studies illustrated the
genetic relationship between schizophrenia and
schizoaffective disorder
Rate among the family members of patients
with schizophrenia can be as high as 9 percent,
general population (less than 1 percent).
20.
20
• One articlepublished way back in 1982 in The
British Journal of Psychiatry reported identical
triplets aged 28, who were discordant by major
Kraepeliniantype of psychosis. Two of them had
been diagnosed schizophrenic while the third was
diagnosed manic depressive.
• One study published in Am J Psychiatry, April 2002
examined 77 monozygotic and 89 same-sex
dizygotic twin pairs in which the proband met the
Research DiagnosticCriteria (RDC) for lifetime-ever
schizophrenic, schizoaffective, or manic syndrome
from the Maudsley Twin Register in London
21.
21
Schizophrenia-Spectrum Personality Disorders
•Schizotypal personality disorder shows the
strongest familial link with schizophrenia
• 1.5 to 5.0 times higher among the relatives of
schizophrenic patients than in the relatives of
controls or in the general population
• Paranoid and schizoid personality disorders
have not provided a similar level of evidence
for a familial association with schizophrnia
22.
22
Schizotaxia
• Conceptualized asthe genetic liability toward
schizophrenia
• Relatively common among the nonpsychotic
relatives of patients with schizophrenia
• Core symptoms of schizotaxia range from 20
to 50 percent among the first-degree relatives
of schizophrenic patients
23.
23
PATHOLOGY
• Brain Structure
Structuralabnormalities exist in a plethora of
cortical and subcortical brain structures in
schizophrenic patients
Increased volume in the lateral ventricles
Decreased volumes in the dorsolateral and medial
prefrontal cortices, cingulate paracingulate cortices,
hippocampus, parahippocampal and superior
temporal gyri, septum pellucidum, and thalamus
24.
24
Brain in schizoaffectivedisorder
• Mixed evidence for common morphology
• Striatal enlargement and cerebral volume
reductions) were each noted in only one of
three existing studies of schizoaffective
patients
• Ventricular enlargement, characteristic of
schizophrenia, was observed in two of three
studies
25.
25
Schizotypal personality disorder
•Abnormalities in the superior temporal and
parahippocampal gyri, lateral ventricles, thalamus, and
septum pellucidum similar to those seen in people with
schizophrenia
• Frontal cortical volume, on the other hand, appears to be
relatively preserved in initial studies of schizotypal
personality disorder
• Medial temporal lobe abnormalities and lateral ventricular
enlargement are not prominent in schizotypal personality
disorder
27
Brain Function
• Schizotypalpersonality disorder
Abnormalities in frontal activation mimic those of
schizophrenia, with the difference that additional
brain regions are recruited to accomplish tasks
requiring frontal lobe activation.
Performance of a verbal working memory task (a
domain that is among the most impaired in schizophrenic patients and
among their nonpsychotic relatives), exhibit reduce activation
relative to controls.
28.
28
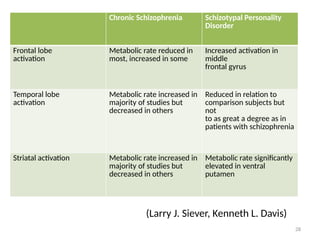
(Larry J. Siever,Kenneth L. Davis)
Chronic Schizophrenia Schizotypal Personality
Disorder
Frontal lobe
activation
Metabolic rate reduced in
most, increased in some
Increased activation in
middle
frontal gyrus
Temporal lobe
activation
Metabolic rate increased in
majority of studies but
decreased in others
Reduced in relation to
comparison subjects but
not
to as great a degree as in
patients with schizophrenia
Striatal activation Metabolic rate increased in
majority of studies but
decreased in others
Metabolic rate significantly
elevated in ventral
putamen
29.
29
Nonpsychotic relatives ofpatients with
schizophrenia, (which also contains individuals
with schizotaxia)
• Abnormal brain activation patterns while
performing working memory tasks
• Such tasks normally produce activation in the
lateral and medial prefrontal cortex, posterior
parietal and thalamus
• Relatives exhibit more bilateral activation on
working memory tasks, than do control
subjects
30.
30
• . Thesefindings indicate at least one or both
of two possibilities:
(1) Relatives demonstrate a compensatory
exertion of inefficient neural circuitry in
attempting to perform an effortful task to
produce accurate output
(2) they have abnormal connectivity in the
circuitry required to perform these tasks.
32
Psychophysiological correlates orintermediate
phenotypes for schizophrenia and schizotypal
personality disorder
• 1. A failure of P50 suppression
• 2. Deficits in prepulse inhibition, which may
impair appropriate modulation of
responsiveness to the environment
• 3. Impairment of smooth-pursuit eye
movements, reflecting involuntary attention
33.
33
• 4. Errorsin antisaccade tasks, which test saccadic
inhibition
• 5. Poor performance on a backward masking task
that assesses early visual processing
• 6. Reduced P300-evoked potentials, which
measure auditory attention
• 7. Performance on the Continuous Performance
Test, a sustained attentional task
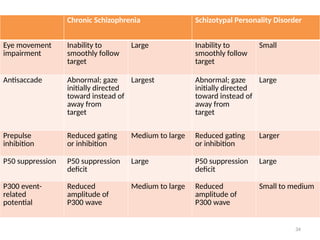
34.
34
Chronic Schizophrenia SchizotypalPersonality Disorder
Eye movement
impairment
Inability to
smoothly follow
target
Large Inability to
smoothly follow
target
Small
Antisaccade Abnormal; gaze
initially directed
toward instead of
away from
target
Largest Abnormal; gaze
initially directed
toward instead of
away from
target
Large
Prepulse
inhibition
Reduced gating
or inhibition
Medium to large Reduced gating
or inhibition
Larger
P50 suppression P50 suppression
deficit
Large P50 suppression
deficit
Large
P300 event-
related
potential
Reduced
amplitude of
P300 wave
Medium to large Reduced
amplitude of
P300 wave
Small to medium
35.
35
NEUROPSYCHOLOGICAL IMPAIRMENT IN
SCHIZOTAXIA
•Motor ability- in children, disturbed gait
• Perceptual motor speed- slow both in adults and
children
• Verbal ability and language- significant impairment both
in children and adults
• Visuo-spatial learning- most studies show no impairment
36.
36
Neurotransmission
• Schizophrenic patientsoften show lower levels of
dopamine-β-hydroxylase (the enzyme that converts
3,4-dihydroxyphenylalanine to dopamine) and
lower plasma levels of homovanillic acid (a
dopamine metabolite).
• Elevated levels of homovanillic acid in schizophrenia
are associated primarily with positive symptoms
• Inverse relationship with negative symptoms (i.e.,
higher levels of negative symptoms associated with
lower levels of homovanillic acid).
37.
37
Studies on neurotransmissionin schizotypal
personality disorder.
• CSF levels of homovanillic acid were increased
among patients with schizotypal personality
disorder relative to controls
• Relationship between lowered homovanillic
acid levels and negative symptoms and
elevated homovanillic acid levels and positive
symptoms
38.
38
Studies of schizotypalindividuals,studies
of nonpsychotic,nonschizotypal relatives
of schizophrenic patients
• Lower circulating levels of homovanillic acid
when compared with a normal control group
• Plasma homovanillic acid is also inversely
correlated with negative symptom scores
39.
39
Proposed Pathophysiological Model
ofthe Spectrum Disorders
• Distinct susceptibilities to the schizophrenia spectrum
and psychosis
• Common genetic anomaly that renders the temporal
cortex particularly vulnerable to environmental insults
such as hypoxia
• Genetic factors and/or favorable environmental
influences would leave the schizotypal individual better
buffered with regard to frontal volume and function as
well as stabilization of subcortical dopaminergic activity
40.
40
• Frontal reservecapacity or, at a cognitive
level, general intelligence
• social deficits and cognitive impairment
characteristic of the entire spectrum of
schizophrenia-related disorders
• is the result of an underlying genetic diathesis
that, in conjunction with modifying
environmental factors
41.
41
• Adversely affectscortical structures such as the
temporal and prefrontal cortex
• Sensitive to developmental aberrations such as
altered migration of neurons, aberrant dendritic
growth patterns, or alterations in the compaction
and maintenance of the myelin sheaths of axons
• Subsequent disconnection between critical brain
regions
42.
42
Increased prefrontal
cortical compensatory
capacitybuffers against
effects of temporal deficits
Temporal lobe
Frontal lobe
Basal ganglia
Early temporal lesions lead to
prefrontal functional deficits
Frontal hypodopaminergia leads to
striatal hyperdopaminergia
---
Disruption of
striatal excitatory
and inhibitory
circuits leads to
cortical dysfunction
43.
43
• Greater frontalreserves in schizotypal personality
disorder compared to schizophrenia protect the
schizotypal individual from the severe cognitive
deterioration and social deficits associated with
chronic schizophrenia.
• Schizotypal individuals may also be able to better use
their frontal capacities
• Compensate for dysfunction in regions such as the
dorsolateral prefrontal cortex, to accomplish working
memory and executive tasks, by activating other
frontal regions not normally recruited by normal
volunteers
44.
44
• Finally, subcorticalstructures that are modulated by
the frontal cortex may be better protected compared
to schizophrenia subjects
• Perhaps because frontal function is better preserved
and/or because intrinsic dopamine activity in the
striatum may be more effectively regulated.
• Comparable individual differences between people
might also modulate the degree to which striatal
dopaminergic up-regulation occurs in the face of
frontal dysfunction, for example, as may be induced
by stress paradigms
45.
45
ENDOPHENOTYPE EXPLANATION
• Evaluationof intermediate phenotypes or
endophenotypes that are common to the
entire spectrum of schizophrenia disorders
• Reflect a genetic impairment, particularly
prominently expressed in temporal or
hippocampal regions, that is common to the
entire schizophrenia spectrum
46.
46
• P50 suppressionabnormality, which is
associated with the alpha-7 nicotinic receptor
gene in relatives of patients with
schizophrenia and reflects an abnormality in
sensory gating or filtering function of the
hippocampus, where these receptors are
localized
47.
47
• Hippocampal impairmentmight lead to P50
abnormalities and perhaps spectrum pathology
but not necessarily schizophrenia
• Predispositions to neurodevelopmental
aberration in the hippocampus or the temporal
cortex, frontal dysfunction may interact
synergistically to increase the probability of
developing schizophrenia
48.
48
• Vulnerability andprotective factors within a
single domain, e.g., hippocampal function
• Relatives of schizophrenia probands with P50
abnormalities have been found to have larger
hippocampi than those without the P50
abnormality
• Consistent with the hypothesis that larger
hippocampi reflecting increased processing
capacity may partially compensate for the
sensory gating deficit in these relatives, thus
protecting them from schizophrenia
49.
49
Future Directions
1. Newopportunities to disentangle the genetics
and pathophysiology of schizophrenia
2. Candidate genes begin to be identified in relation
to schizophrenia disorders , the genes that are
associated with both schizotypal and
schizophrenia disorders and those that are unique
to schizophrenia and psychosis may be identified
50.
50
3. To provideintermediate phenotypes to more
finely hone our understanding of the
character of genetic or phenomenological
relationships in the spectrum
4. Opportunity to pilot pharmacological
interventions to enhance cognitive function
or improve negative symptoms
52
Bibliography
• Comprehensive Textbookof Psychiatry, Kaplan & Sadock, 8th
Edition
• Am J Psychiatry 2004; 161:398–413; The Pathophysiology of
Schizophrenia Disorders: Perspectives From the Spectrum; Larry J.
Siever, M.D.,Kenneth L. Davis, M.D.
• Comprehensive Textbook of Psychiatry, Kaplan & Sadock, 9th
Edition
• Neurobiology of Schizophrenia Spectrum Disorders ;Stephan
Heckers; Annals Academy of Medicine; May 2009, Vol. 38 No. 5
Editor's Notes
#12 Characteristic symptoms: Two (or more) of the following, each present for a significant portion of time during a 1-month period (or less if successfully treated):
(1) Delusions
(2) Hallucinations
(3) Disorganized speech
(4) Grossly disorganized or catatonic behavior
(5) Negative symptoms, i.e., affective flattening, alogia, or avolition
Note: Only one Criterion A symptom is required if delusions are bizarre or hallucinations consist of a voice keeping up a running commentary on the person's behavior or thoughts, or two or more voices conversing with each other
schizoaffective disorder shares more than any other disorder in common with schizophrenia clinically.
. Of the two subtypes of schizoaffective disorder, the depressive type is believed to lie nearer the schizophrenia
Nevertheless, there is evidence that both subtypes are on a disease continuum that includes schizophrenia, suggesting that the traditional boundary between schizophrenia and mood disorders may be somewhat artificial
#17 Schizophrenia includes behavioyr contents , learned not inherited
Schizotaxic by social learning develops schizotypal disorder
#19 clinical similarity to schizophrenia clearly identifies several disorders that can be assigned to the schizophrenia spectrum with varying degrees of certainty based on the extent of their similarity to schizophrenia. Schizoaffective disorder is at the top of this list and schizoid and paranoid personality disorders at the bottom
additional standards are helpful in making the distinction between conditions that merely share some symptoms with schizophrenia
#23 pathology of schizophrenia is complex and elusive
#32 The P50 is the positive component of the event-related potential that occurs about 50 msec after an auditory stimulus. The change in P50 amplitude is typically measured as response to click pairs separated by 500 msec. The percentage of the amplitude reduction of the P50 response from the first to the second click is the dependent variable, P50 suppression. Patients with schizophrenia have significantly lower than normal levels of P50 suppression, an operational measure of sensory gating (for reviews, see references 1 and 2).
The human startle reflex is typically assessed by using electromyographic (EMG) recordings of the eye-blink component of the startle reflex in response to sudden and powerful multimodal stimuli, most often acoustic stimuli. When the startling stimulus is preceded by a weak prestimulus (i.e., "prepulse"), the magnitude of the eye-blink response is normally reduced. The percentage of the reduction in the startle reflex is the operational measure of sensorimotor gating known as "prepulse inhibition." As with P50 suppression, patients with schizophrenia often have low levels of prepulse inhibition (for reviews, see references 1 and 2).
#36 it has been difficult to establish whether these dopaminergic abnormalities precede the illness and contribute to its genesis or are a consequence of psychosis or pharmacological treatments.
#38 differences between these individuals and normal controls can be viewed as a consequence of the underlying predisposition toward illness
#39 genetic factors independent of the vulnerability to the schizophrenia spectrum per se and/or more favorable environmental influences would leave the schizotypal individual better buffered with regard to frontal volume and function as well as stabilization of subcortical dopaminergic activity
#50 Opportunity to pilot pharmacological interventions that might serve to enhance cognitive function or improve negative symptoms because these individuals have more reversible cognitive and social deficits than patients with chronic schizophrenia and are less vulnerable to potential worsening of psychosis







![Revised Topic- Schizophrenia [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/schizophreniaautosaved-250310073514-5d1607b2-thumbnail.jpg?width=640&height=640&fit=bounds)









![schizophrenia_-final[1]psychiatry courses.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/schizophrenia-final1-241125165758-037ddbda-thumbnail.jpg?width=640&height=640&fit=bounds)































