OUTLINE OF THEREPORT
:
I. Introduction
II. History
III. Epidemiology
IV. Etiology
V. Psychosocial
and psychoanalytic
theories
VI. Diagnosis &
their subtypes
VII. Clinical features
VIII.Mental status examination
IX. Differential diagnosis
X. Course and prognosis
XI. Treatment
XII. Managing side effects
XIII.Other biological therapies
3.
I. INTRODUCTION
• Schizophreniais a common of the serious mental/psychiatric disorders, but its
essential nature remains to be clarified thus, it is sometimes referred to as a
syndrome, as the group of schizophrenias, or as in the fifth edition of the diagnostic
and statistical manual of mental disorders (DSM-5), the schizophrenia spectrum..
• Constellation of abnormalities in thinking, emotion,
and behavior.
• No single symptom that is pathognomonic
• Schizophrenia is typically chronic, with significant psychosocial
and medical consequences to the patient.
• Diagnosis of schizophrenia based - psychiatric history and
mental status examination.
• There is no laboratory test for schizophrenia.
4.
• Emil Kraepelin:Kraepelin identified manic depression and
dementia praecox, later termed as schizophrenia, as distinct forms
of psychosis.
• Eugene Bleuler: Bleuler always believed that schizophrenia was
an organic illness and that it could be inherited.
The four are ;
Bleuler identified specific fundamental symptoms for the
diagnosis of schizophrenia.
• Associational Disturbances Of Thought,
• Affective Disturbances,
• Autism,
• Ambivalence
The other symptoms are hallucination and delusion, these are
known as secondary symptoms.
HISTORY ;
5.
Other Theorists ;
ErnstKretschmer (1888–1926); Schizophrenia occurred more
often among persons with asthenic (i.e. slender, lightly muscled
physiques), athletic or dysplastic body type rather than with pyknic
(i.e. short, stocky physiques) body types.
• Pyknic body types – bipolar disorders
Adolf Meyer (1866–1950); Founder of psychobiology
• Schizophrenia – reaction to life stresses; maladaptation in terms
of the patient’s life experiences (schizophrenic reaction – 1950s).
HISTORY ;
6.
The lifetime prevalenceof schizophrenia is about 1 percent, which
means that about one person in 100 will develop schizophrenia
during their lifetime.
Gender and Age-Schizophrenia is equally prevalent in men and
women. The two genders differ, however, in the onset and course
of illness. Onset is earlier in men than in women.
Medical Illness -Persons with schizophrenia have a higher
mortality rate from accidents and natural causes than the general
population. Institution- or treatment-related variables do not explain
the increased mortality rate.
Infections and birth season-Persons who develop schizophrenia
are more likely to have been born in the winter and early spring and
less likely to have been born in late spring and summer
EPIDEMOLOGY;
7.
Substance Abuse- Substanceabuse is common in
schizophrenia.
Nicotine. Up to 90 percent of schizophrenia patients
may be dependent on nicotine
Population Density -social stressors in urban
settings may affect the development of schizophrenia
in persons at risk
Socioeconomic and Cultural Factors-
Economics. Because schizophrenia begins early in
life; causes significant and long-lasting impairments
EPIDEMOLOGY;
• The causesof schizophrenia are not known.
• 2 sets of risk factors, genetic and perinatal.
• Undefined socioenvironmental factors may increase the risk of schizophrenia in
international migrants or urban populations of ethnic minorities.
• Increased paternal age is associated with a greater risk of schizophrenia.
ETIOLOGY
10.
PSYCHOSOCIAL AND PSYCHOANALYTICTHEORIES ;
Psychoanalytic Theories :
⮚ Sigmund Freud : Developmental fixations in early life – Resulting defects in ego
development – Symptom of schizophrenia.
⮚ Margaret Mahler : Distortions in the reciprocal relationship between the infant and the
mother.
⮚ Paul Federn : Defect in ego functions permits intense hostility and aggression to
distort the mother-infant relationship – personality disorganization and vulnerability to
stress.
⮚ Harry Stack Sullivan : Schizophrenia as a disturbance in interpersonal relatedness.
According to him, schizophrenia is an adaptive method used to avoid panic, terror,
and disintegration of the sense of self - anxiety results from cumulative
experiential traumas during development.
11.
PSYCHOSOCIAL AND PSYCHOANALYTICTHEORIES ;
Psychoanalytic Theories :
⮚ All psychodynamic approaches are founded on the premise that psychotic symptoms
have meaning in schizophrenia .
⮚ Psychoanalytic theory postulates various symptoms of schizophrenia have symbolic
meaning for individual patients.
• Example : Fantasies of the world coming to an end may indicate a perception that a
person's internal world has broken down.
Feelings of inferiority are replaced by delusions of grandeur and
omnipotence.
Hallucinations may be substitutes for a patient's inability to deal with
objective reality and may represent inner wishes or fears.
Delusions, similar to hallucinations, are regressive, restitutive attempts to
create a new reality or to express hidden fears or impulses
13.
Learning theory :
•The poor interpersonal relationships of persons with schizophrenia develop because of poor
models for learning during childhood.
Family Dynamic : ((stress that may reveal vulnerability to or exacerbate psychosis) )
• Poor mother-child relationship - sixfold increase in the risk of developing schizophrenia.
• Double Bind [Gregory Bateson and Donald Jackson] - Children receive conflicting parental
messages about their behavior, attitudes, and feelings. In bateson's hypothesis, children withdraw
into a psychotic state to escape the unsolvable confusion of the double bind.
An example of a double bind is a parent who tells a child to provide cookies for his or her friends and then
chastises the child for giving away too many cookies to playmates.
14.
• Schisms andSkewed Families [Theodore Lidz] – 2 Abnormal patterns of family behavior.
1) In 1 family type - prominent schism between the parents, one parent is overly close to a child of the
opposite gender.
2) In the other family type, a skewed relationship between a child and one parent involves a power struggle
between the parents and the resulting dominance of one parent.
15.
PSYCHOSOCIAL AND PSYCHOANALYTICTHEORIES ;
• Pseudomutual and Pseudohostile Families [Lyman Wynne] - Suppress emotional expression by
consistently using pseudomutual or pseudohostile verbal communication.
• The child's verbal communication may be incomprehensible to outsiders.
• Expressed Emotion - Parents or other caregivers may behave with ;
✔Over criticism
✔Hostility
✔ over involvement toward a person with schizophrenia
• Families with high levels of expressed emotion (hostile critical and controlling), the relapse rate for
schizophrenia exacerbation is high.
16.
5 subtypes ofschizophrenia have been described based predominantly on clinical presentation:
Paranoid Type. The paranoid type of schizophrenia is characterized by preoccupation with one or
more delusions or frequent auditory hallucinations.
Disorganized Type. The disorganized type of schizophrenia is characterized by a marked
regression to primitive, disinhibited, and unorganized behavior
DIAGNOSIS AND THEIR SUBTYPES
17.
Catatonic Type.- Theclassic feature of the catatonic type is a marked disturbance in motor function; this
disturbance may involve stupor, negativism, rigidity, excitement, or posturing.
Undifferentiated Type. Frequently, patients who clearly have schizophrenia
cannot be easily fit into one type or another
Residual Type. The residual type of schizophrenia is characterized by continuing evidence of the schizophrenic
disturbance in the absence of a complete set of active symptoms or of sufficient symptoms to meet the diagnosis of
another type of schizophrenia.
18.
The clinical signsand symptoms of schizophrenia raises three key issues.
• No clinical sign or symptom for schizophrenia;every sign or symptom seen in
schizophrenia occurs in other psychiatric and neurological disorders. Therefore, a
patient's history is essential for the diagnosis of schizophrenia.
• Patient's symptoms change with time. For example, a patient may have intermittent
hallucinations and a varying ability to perform adequately in social situations, or
significant symptoms of a mood disorder may come and go during the course of
schizophrenia.
• Third, clinicians must take into account the patient's educational land intellectual ability.
An impaired ability to understand abstract concepts, for example, may reflect either the
patient's education or his or her intelligence.
CLINICAL FEATURES:
20.
MENTAL STATUS EXAMINATION;
General Description :
• Appearance: Completely disheveled, screaming, agitated person to an obsessively groomed,
completely silent, and immobile person.
• Talkative and may exibit bizarre postures.
• Behavior : agitated or violent, apparently in an unprovoked manner, but usually in response
to hallucinations.
• In contrast, in catatonic stupor, often referred to as catatonia- patients seem completely
lifeless
• They may exhibit such signs as muteness, negativism, and automatic obedience.
• Waxy flexibility - common sign in catatonia - manneristic behavior( A person with a less
extreme subtype of catatonia may show marked social withdrawal and egocentricity, a lack of
spontaneous speech or movement, and an absence of goal-directed behavior).
• Relatedness: often impaired (e.g. Precox Feeling - an intuitive experience of their inability to
establish an emotional rapport with a patient)
21.
• Mood/Affect: Reducedemotional responsiveness, sometimes severe enough to warrant the label of
anhedonia, and overly active or inappropriate emotions such as extremes of rage, happiness, and anxiety.
• emotional patient - exultant feelings of omnipotence, religious ecstasy, terror at the disintegration of their
souls, or paralyzing anxiety about the destruction of the universe.
• Other feeling tones include perplexity, a sense of isolation, overwhelming ambivalence, and depression.
Perceptual Disturbances
Hallucinations :
• Auditory - with voices that are often threatening, obscene, accusatory, or insulting.
• Visual hallucinations - tactile, olfactory, and gustatory hallucinations are unusual.
• Cenesthetic hallucinations - Unfounded sensations of altered states in bodily organs; als,o fairly
common.
Illusions : distortions of real images or sensations, hallucinations are not based on real images or
sensations.
• Illusions - occur in schizophrenia patients during active phases,also in prodromal phases and
periods of remission.
MENTAL STATUS EXAMINATION ;
22.
Thought Disorder :core symptoms of schizophrenia.
Dividing the disorders of thought into ;
I. Thought content,
II. Form of thought, and
III. Thought process is one way to clarify them.
Thought content: Reflect patient's ideas, beliefs, and interpretations of stimuli.Example ;
Delusions.
• loss of ego boundaries - lack of a clear sense of where the patient's own body, mind, and
influence end and where those of other animate and inanimate objects begin.
• For example, patients may think that other persons, the television, or the newspapers are
referring to them (ideas of reference ).
MENTAL STATUS EXAMINATION ;
23.
Form of Thought: objectively observable in patients' spoken and written language.
• The disorders include looseness of associations, derailment, incoherence, tangentiality,
circumstantiality, neologisms, echolalia, verbigeration, word salad, and mutism.
Thought Process : It concern the way ideas and languages are formulated. The examiner infers a
disorder from what and how the patient speaks, writes, or draws.
• The examiner may also assess the patient's thought process by observing his or her behavior,
especially in carrying out discrete tasks (e.g., in occupational therapy).
Impulsiveness, Violence, Suicide and Homicide.
Sensorium and Cognition
• Orientation - oriented to person, time, and place. And possibility of a medical or neurological brain
disorder
• Memory- usually intact, but there can be minor cognitive deficiencies.
• Cognitive Impairment
• Judgment and Insight
• Reliability
MENTAL STATUS EXAMINATION ;
24.
Somatic Comorbidity
• NeurologicalFindings
✔Localizing and nonlocalizing neurological signs
• Eye examination - The elevated blink rate is believed to reflect hyperdopaminergic activity.
• Speech - Inability to perceive the prosody of speech or to inflect their own speech can be
seen as a neurological symptom of a disorder in the nondominant parietal lobe.
Other Comorbidities
• Obesity
• Diabetes Mellitus
• Cardiovascular Disease
• HIV
• Chronic Obstructive Pulmonary Disease
• Rheumatoid Arthritis
MENTAL STATUS EXAMINATION ;
25.
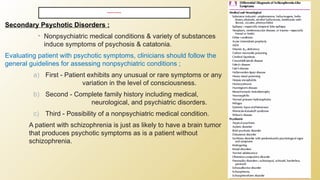
DIFFERENTIAL DIAGNOSIS
Secondary PsychoticDisorders :
• Nonpsychiatric medical conditions & variety of substances
induce symptoms of psychosis & catatonia.
Evaluating patient with psychotic symptoms, clinicians should follow the
general guidelines for assessing nonpsychiatric conditions ;
a) First - Patient exhibits any unusual or rare symptoms or any
variation in the level of consciousness.
b) Second - Complete family history including medical,
neurological, and psychiatric disorders.
c) Third - Possibility of a nonpsychiatric medical condition.
A patient with schizophrenia is just as likely to have a brain tumor
that produces psychotic symptoms as is a patient without
schizophrenia.
26.
COURSE & PROGNOSIS
COURSE:
• Premorbid pattern – 1st
evidence of illness.
• Symptoms begin in adolescence development of prodromal symptoms in days or
🡪
few
months.
• Classic course - Exacerbations and remissions.
• Positive symptoms - Less severe with time.
• Negative or deficit symptoms - ↑severity
• 1/3 of schizophrenia patients - Marginal or integrated social existence, most have
lives characterized by aimlessness; inactivity; frequent hospitalizations; and, in
urban settings, homelessness and poverty.
27.
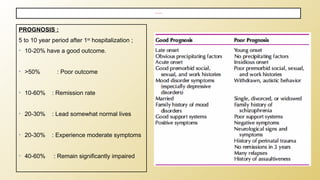
PROGNOSIS :
5 to10 year period after 1st
hospitalization ;
• 10-20% have a good outcome.
• >50% : Poor outcome
• 10-60% : Remission rate
• 20-30% : Lead somewhat normal lives
• 20-30% : Experience moderate symptoms
• 40-60% : Remain significantly impaired
COURSE & PROGNOSIS
28.
⮚ Antipsychotics canbe categorized into two main groups: the older conventional antipsychotics,
which have also been called first generation antipsychotics or dopamine receptor antagonists,
and the newer drugs, which have been called second-generation antipsychotics or serotonin
dopamine antagonists (SDAs).
⮚ Antipsychotics and benzodiazepines can result in relatively rapid calming of patients
⮚ With highly agitated patients, intramuscular administration of antipsychotics produces a more
rapid effect.
⮚ Benzodiazepines are also effective for agitation during acute psychosis. Lorazepam (Ativan)
has the advantage of reliable absorption when it is administered either orally or intramuscularly.
TREATMENT
30.
• Tardive Dyskinesia; About 20 to 30 percent of patients on long-term treatment with
a conventional DRA will exhibit symptoms of tardive dyskinesia.
⮚ Patients with comorbid cognitive or mood disorders may also be more vulnerable to
tardive dyskinesia than those with only schizophrenia
⮚ Electroconvulsive therapy (ECT) has been studied in both acute and chronic
schizophrenia.
⮚ Studies in recent-onset patients indicate that ECT is about as effective as
antipsychotic medications and more effective than psychotherapy
TREATMENT
31.
IMPORTANT SIDE EFFECTSAND
CONSEQUENCES OF ANTIPSYCHOTIC MEDICATIONS
Side effects of antipsychotic medications include:
1. Extrapyramidal symptoms (especially with the use of high-potency firstgeneration antipsychotics):
■ Dystonia (spasms) of face, neck, and tongue.
■ Parkinsonism (resting tremor, rigidity, bradykinesia).
■ Akathisia (feeling of restlessness).
Treatment: anticholinergics (benztropine, diphenhydramine), benzodiazepines/beta-blockers
(specifically for akathisia).
2. Anticholinergic symptoms (especially low-potency first-generation antipsychotics and atypical
antipsychotics): dry mouth, constipation, blurred vision, hyperthermia.
Treatment: as per symptom (eye drops, stool softeners, etc.).
32.
IMPORTANT SIDE EFFECTSAND
CONSEQUENCES OF ANTIPSYCHOTIC MEDICATIONS
3. Metabolic syndrome (second-generation antipsychotics): A constellation of conditions—
elevated blood pressure, elevated blood sugar levels, excess body fat around the waist,
abnormal cholesterol levels—that occur together, increasing the risk for cardiovascular
disease, stroke, and type 2 diabetes.
Treatment: Consider switching to a first-generation antipsychotic or a more “weight-neutral”
second-generation antipsychotic such as aripiprazole or ziprasidone. Consider metformin if the
patient is not already on it. Monitor lipids and blood glucose measurements. Refer the patient
to primary care for appropriate treatment of hyperlipidemia, diabetes, etc. Encourage
appropriate diet, exercise, and smoking cessation.
4. Tardive dyskinesia (more likely with first-generation antipsychotics): Choreoathetoid
movements, usually seen in the face, tongue, and head.
Treatment: Discontinue or reduce the medication and consider substituting an atypical
antispsychotic (if appropriate). VMAT-2 inhibitors such as valbenzazine, benzodiazepines,
Botox, and vitamin E may be used. The movements may persist despite withdrawal of the
drug. Although less common, atypical antipsychotics can also cause tardive dyskinesia.
33.
5. Neuroleptic malignantsyndrome (NMS) (typically high-potency first generation antipsychotics):
■ Change in mental status, autonomic instability (high fever, labile blood pressure, tachycardia,
tachypnea, diaphoresis), “lead pipe” rigidity, elevated creatine kinase (CK) levels, leukocytosis,
and metabolic acidosis. Reflexes are decreased.
■ NMS is a medical emergency that requires prompt withdrawal of all antipsychotic medications
and immediate medical assessment and treatment.
■May be observed in any patient being treated with any antipsychotic (including second
generation) medications at any time, but is more frequently associated with the initiation of
treatment and at higher IV/ IM dosing of high-potency neuroleptics.
■ Patients with a history of prior neuroleptic malignant syndrome are at increased risk of recurrent
episodes when retrialed with antipsychotic agents.
IMPORTANT SIDE EFFECTS AND
CONSEQUENCES OF ANTIPSYCHOTIC MEDICATIONS
34.
• Electroconvulsive therapy
•Psychosocial therapies
• Social skills training
• Family-oriented therapies
• Case management
• Assertive community treatment
• Group therapy
• Cognitive behavioral therapy
• Individual psychotherapy
• Personal therapy
• Dialectical behavior therapy
• Vocational therapy
• Art therapy
• Cognitive training
•
OTHER BIOLOGICAL THERAPIES
35.
DSM 5 CRITERIADIAGNOSTIC CRITERIA :
⮚ The presence of hallucinations or delusions is not necessary for a diagnosis of schizophrenia; the
patient's disorder is diagnosed as schizophrenia when the patient exhibits two of the symptoms
listed in symptoms 1 through 5 of Criterion A
⮚ Criterion B requires that impaired functioning, although not deteriorations, be present during the
active phase of the illness.
⮚ Symptoms must persist for at least 6 months, and a diagnosis of schizoaffective disorder or mood
disorder must be absent
OTHER BIOLOGICAL THERAPIES
37.
• DIFFERENTIAL DIAGNOSIS
▪The psychiatric differential diagnosis includes all the possibilities usually considered for mood
disorders and for schizophrenia. In any differential diagnosis of psychotic disorders, a complete
medical workup should be performed to rule out organic causes for the symptoms.
▪ A history of substance use may indicate a substance-induced disorder.
▪ Preexisting medical conditions, their treatment, or both can cause psychotic and mood
disorders.
▪ Any suspicion of a neurological abnormality warrants consideration of a brain scan to rule out
anatomical pathology and an electroencephalogram to determine any possible seizure
disorders (e.g., temporal lobe epilepsy).
▪ Psychotic disorder caused by seizure disorder is more common than that seen in the general
population.
▪ It tends to be characterized by paranoia, hallucinations, and ideas of reference.
▪ Patients with epilepsy with psychosis are believed to have a better level of function than
patients with schizophrenic spectrum disorders.
▪ Better control of the seizures can reduce the psychosis.
OTHER BIOLOGICAL THERAPIES
![Learning theory :
• The poor interpersonal relationships of persons with schizophrenia develop because of poor
models for learning during childhood.
Family Dynamic : ((stress that may reveal vulnerability to or exacerbate psychosis) )
• Poor mother-child relationship - sixfold increase in the risk of developing schizophrenia.
• Double Bind [Gregory Bateson and Donald Jackson] - Children receive conflicting parental
messages about their behavior, attitudes, and feelings. In bateson's hypothesis, children withdraw
into a psychotic state to escape the unsolvable confusion of the double bind.
An example of a double bind is a parent who tells a child to provide cookies for his or her friends and then
chastises the child for giving away too many cookies to playmates.](https://image.slidesharecdn.com/schizophrenia-part-1-260114120637-0e511d08/85/SCHIZOPHRENIA-PART-1-presentation-lecture-pptx-13-320.jpg)
![• Schisms and Skewed Families [Theodore Lidz] – 2 Abnormal patterns of family behavior.
1) In 1 family type - prominent schism between the parents, one parent is overly close to a child of the
opposite gender.
2) In the other family type, a skewed relationship between a child and one parent involves a power struggle
between the parents and the resulting dominance of one parent.](https://image.slidesharecdn.com/schizophrenia-part-1-260114120637-0e511d08/85/SCHIZOPHRENIA-PART-1-presentation-lecture-pptx-14-320.jpg)
![PSYCHOSOCIAL AND PSYCHOANALYTIC THEORIES ;
• Pseudomutual and Pseudohostile Families [Lyman Wynne] - Suppress emotional expression by
consistently using pseudomutual or pseudohostile verbal communication.
• The child's verbal communication may be incomprehensible to outsiders.
• Expressed Emotion - Parents or other caregivers may behave with ;
✔Over criticism
✔Hostility
✔ over involvement toward a person with schizophrenia
• Families with high levels of expressed emotion (hostile critical and controlling), the relapse rate for
schizophrenia exacerbation is high.](https://image.slidesharecdn.com/schizophrenia-part-1-260114120637-0e511d08/85/SCHIZOPHRENIA-PART-1-presentation-lecture-pptx-15-320.jpg)






![schizophrenia [Autosaved].pptx [mental health nursing]](https://cdn.slidesharecdn.com/ss_thumbnails/schizofinalautosaved-250323084409-0f866c5d-thumbnail.jpg?width=640&height=640&fit=bounds)
















![Revised Topic- Schizophrenia [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/schizophreniaautosaved-250310073514-5d1607b2-thumbnail.jpg?width=640&height=640&fit=bounds)



![schizophrenia_-final[1]psychiatry courses.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/schizophrenia-final1-241125165758-037ddbda-thumbnail.jpg?width=640&height=640&fit=bounds)





















