Download to read offline



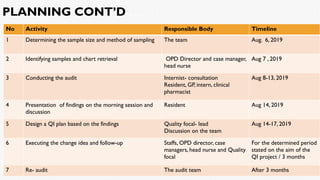









A clinical audit was conducted at St. Peter Specialized Hospital focusing on hypertension management, identifying key stakeholders and collecting data to improve care outcomes. Major gaps highlighted included a lack of standard protocols, poor understanding of treatment guidelines, and inadequate patient follow-up. The audit aimed to increase the percentage of patients with controlled hypertension from 52% to 80% by December 2019 through various quality improvement measures.


























































