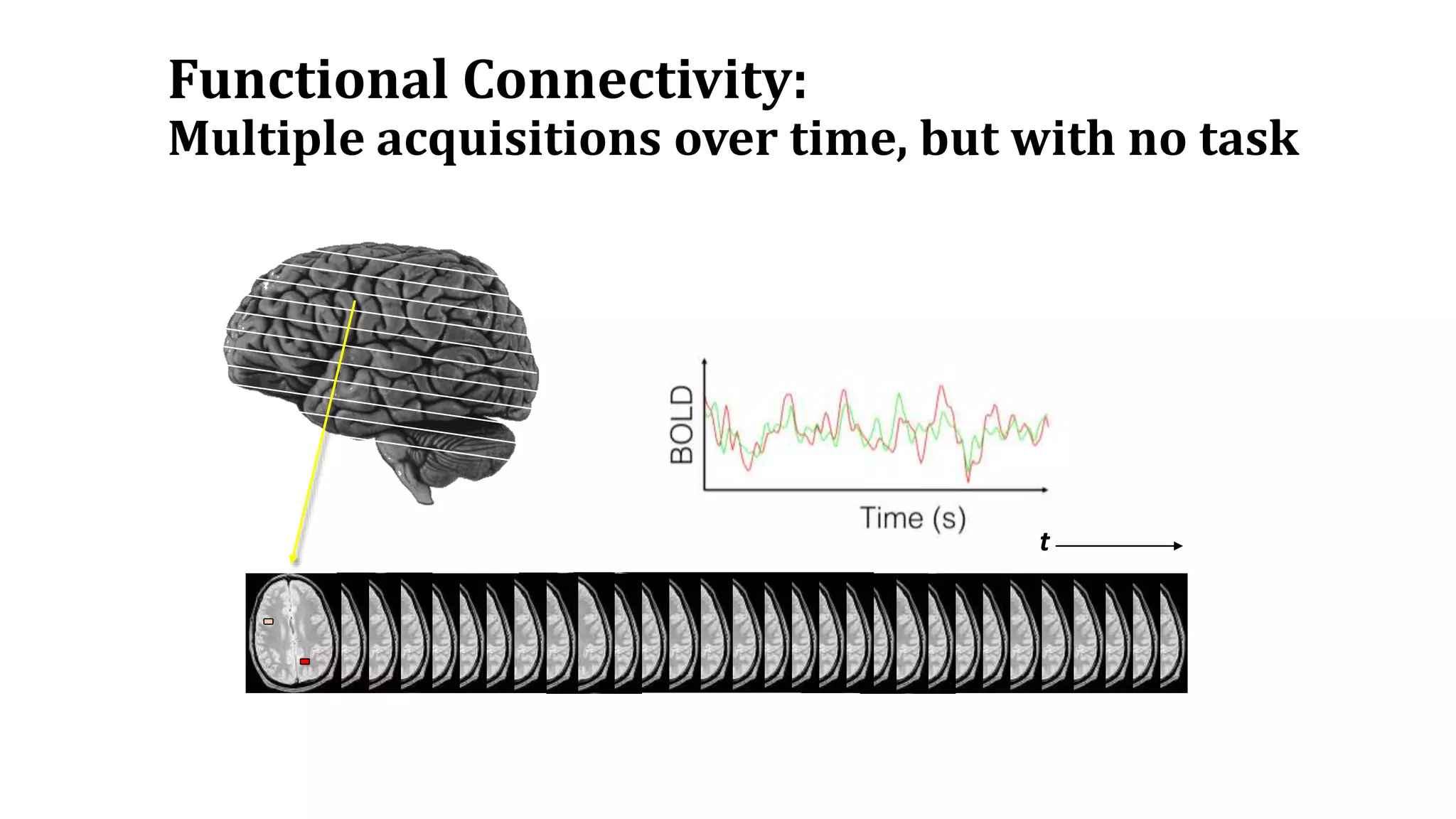
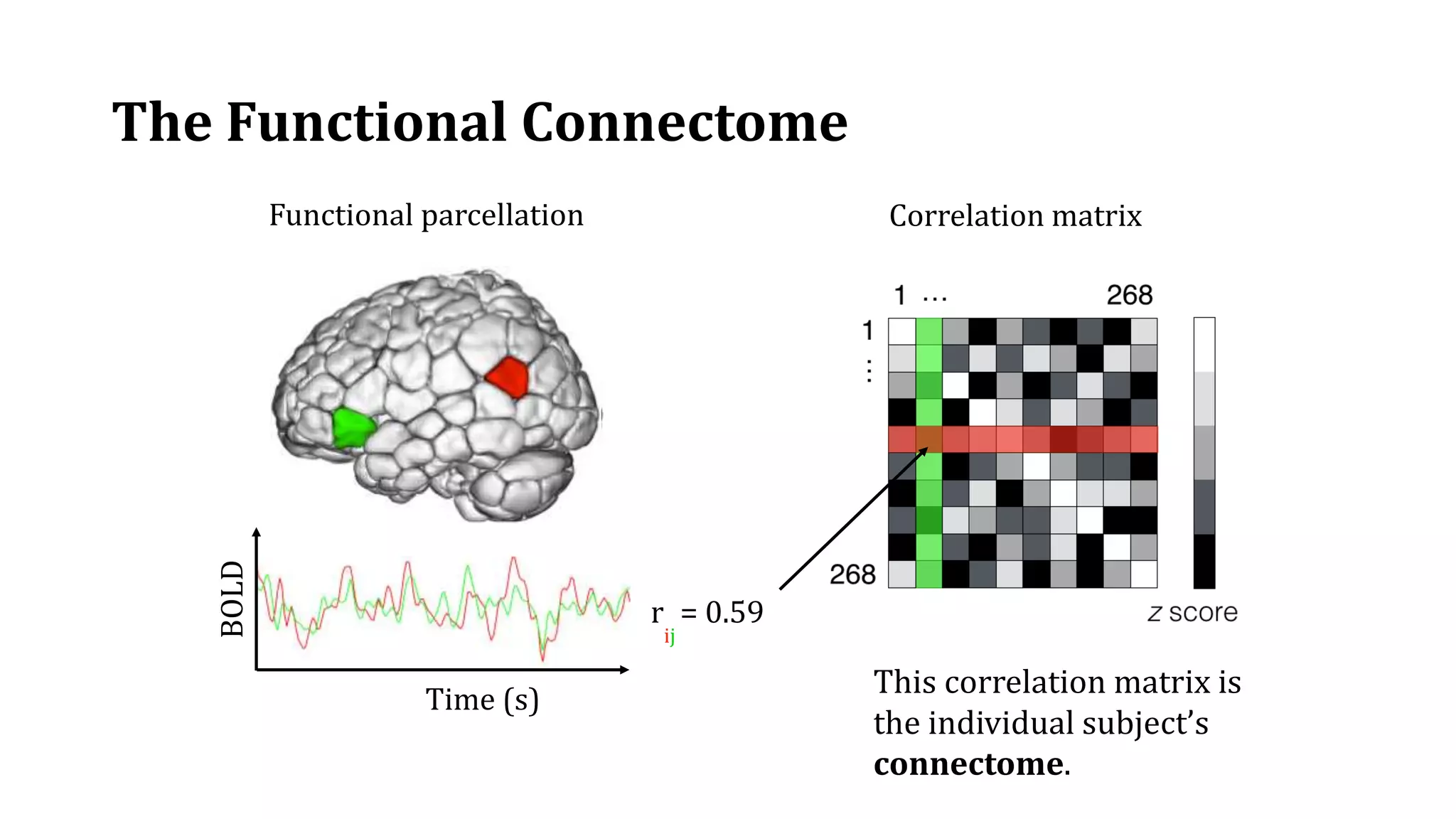
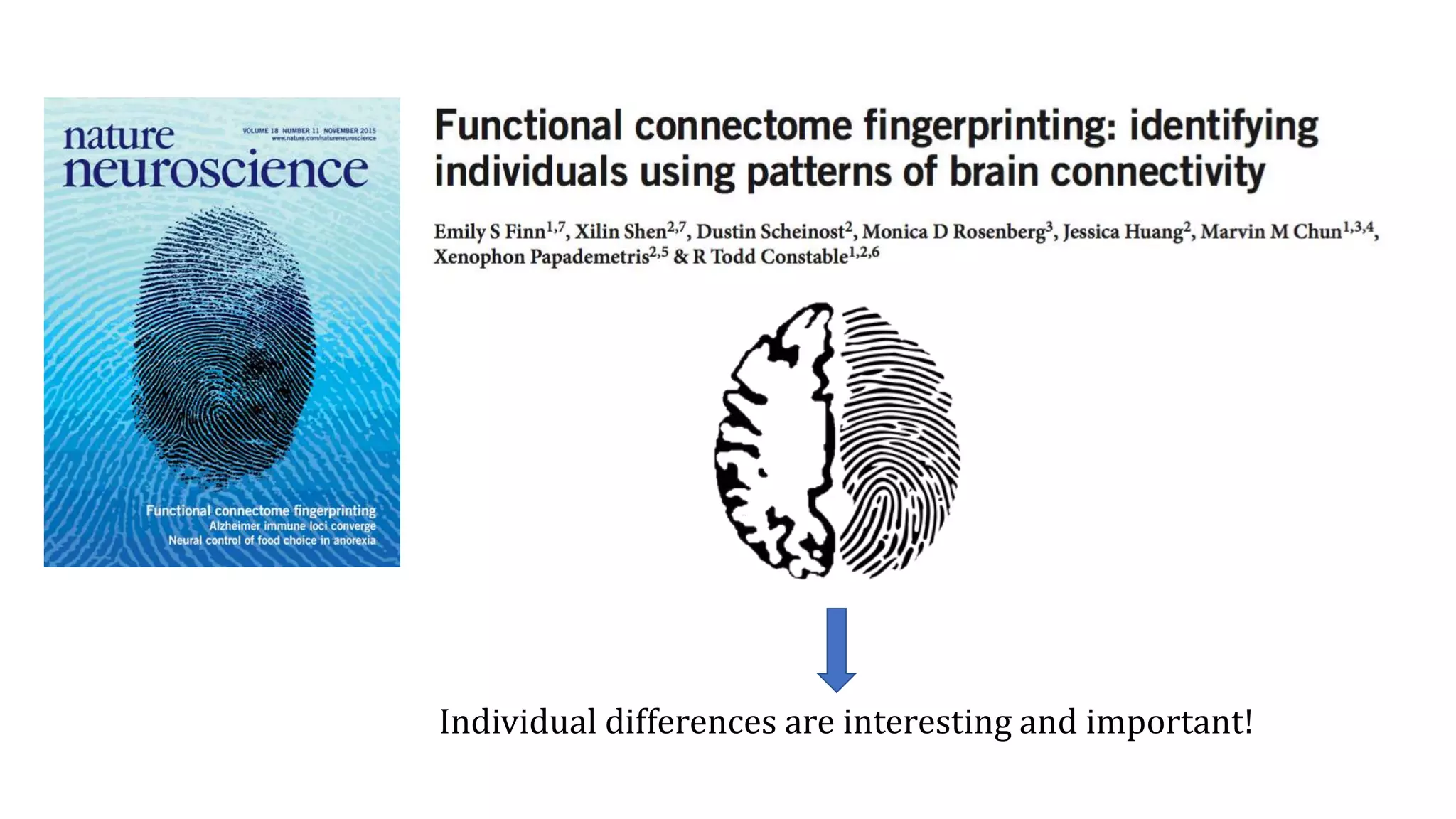
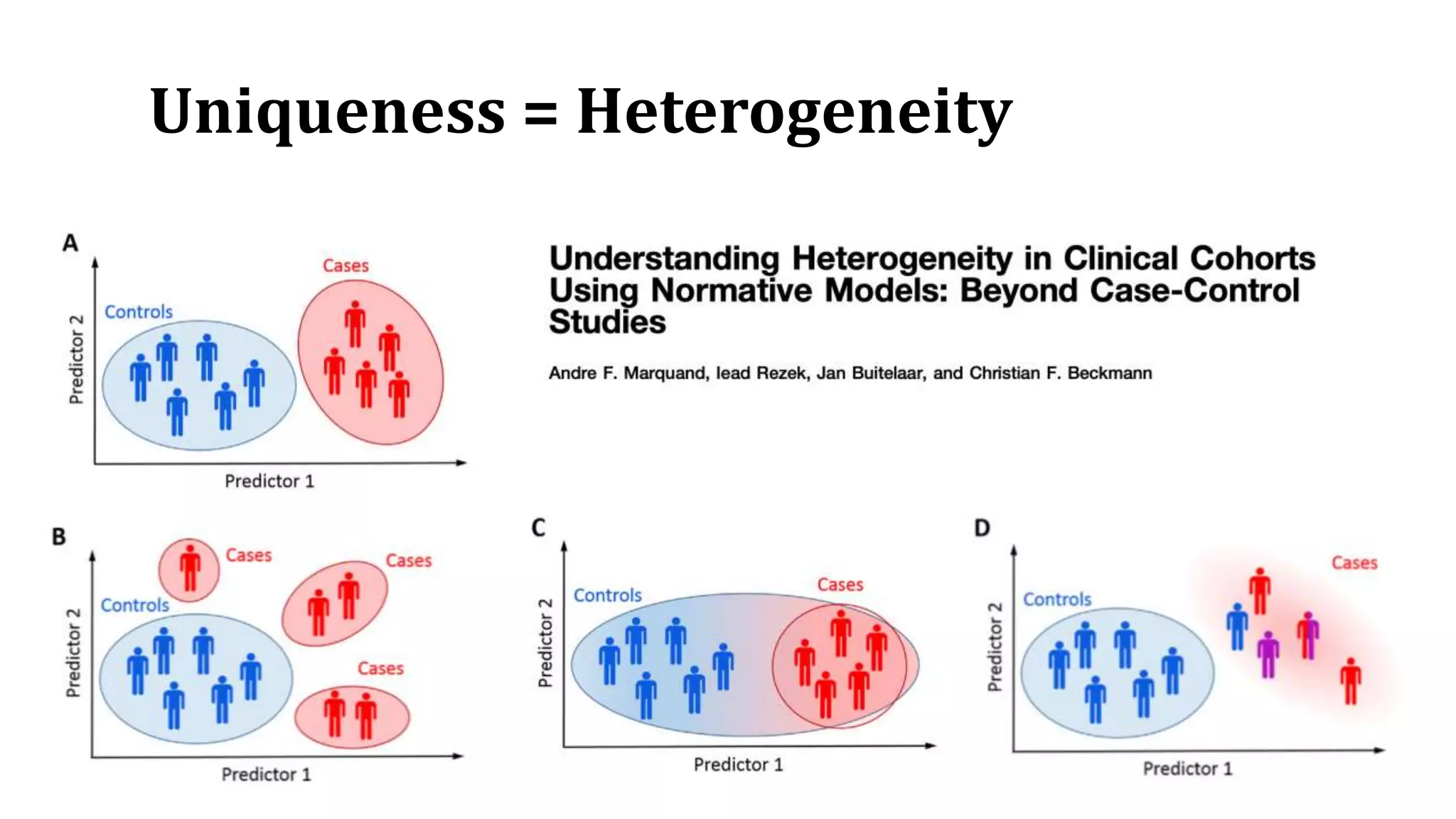
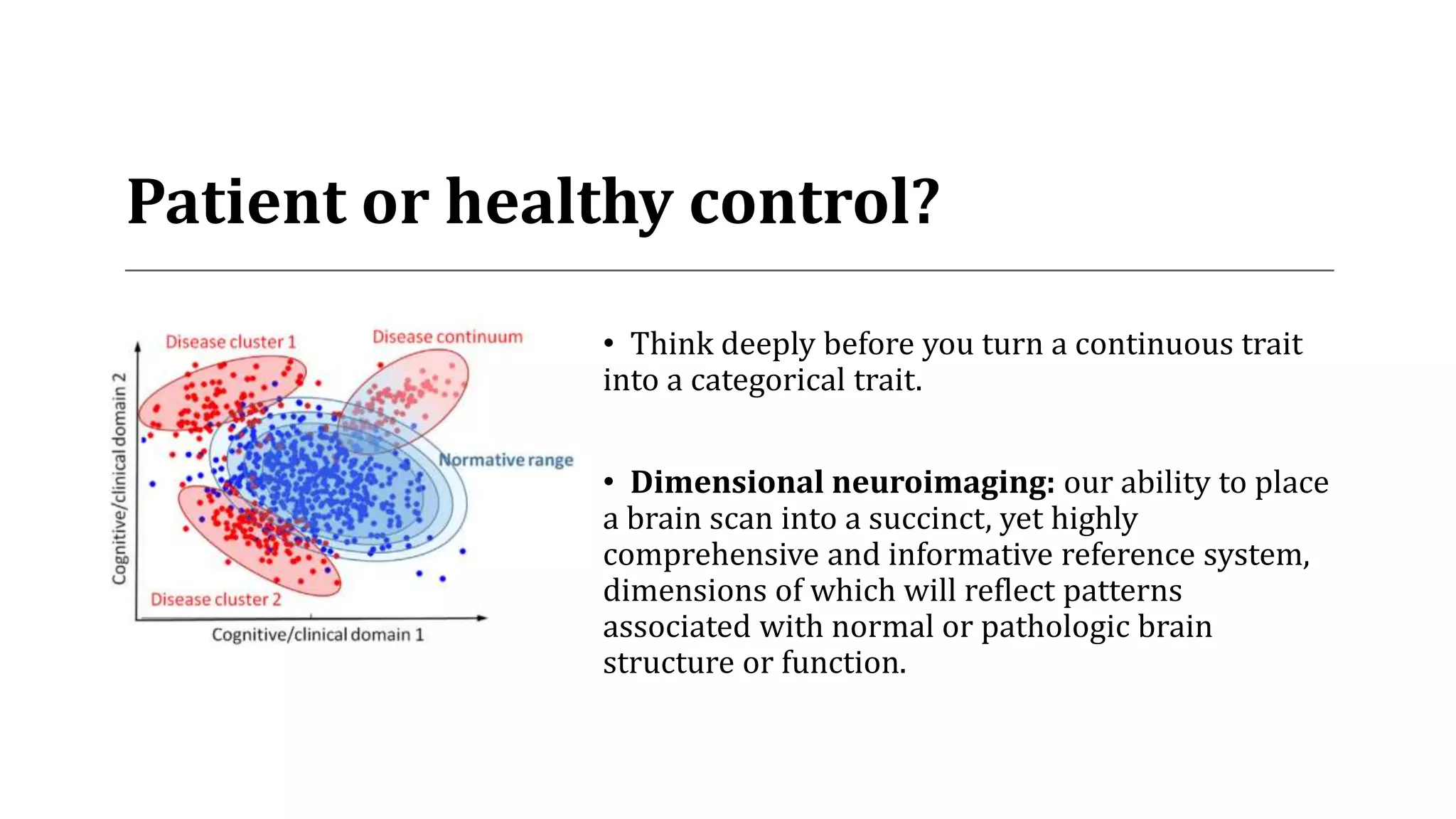
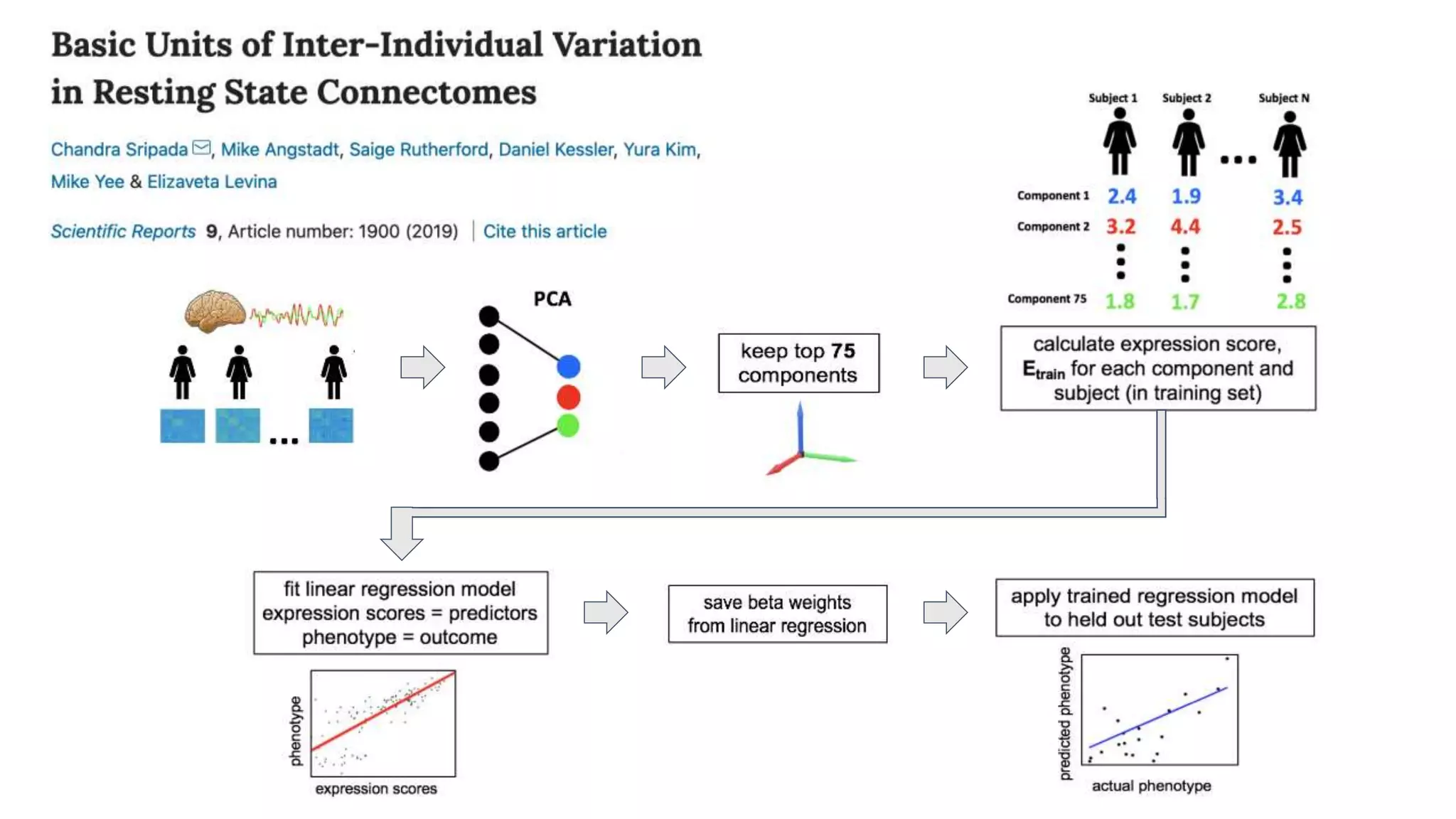
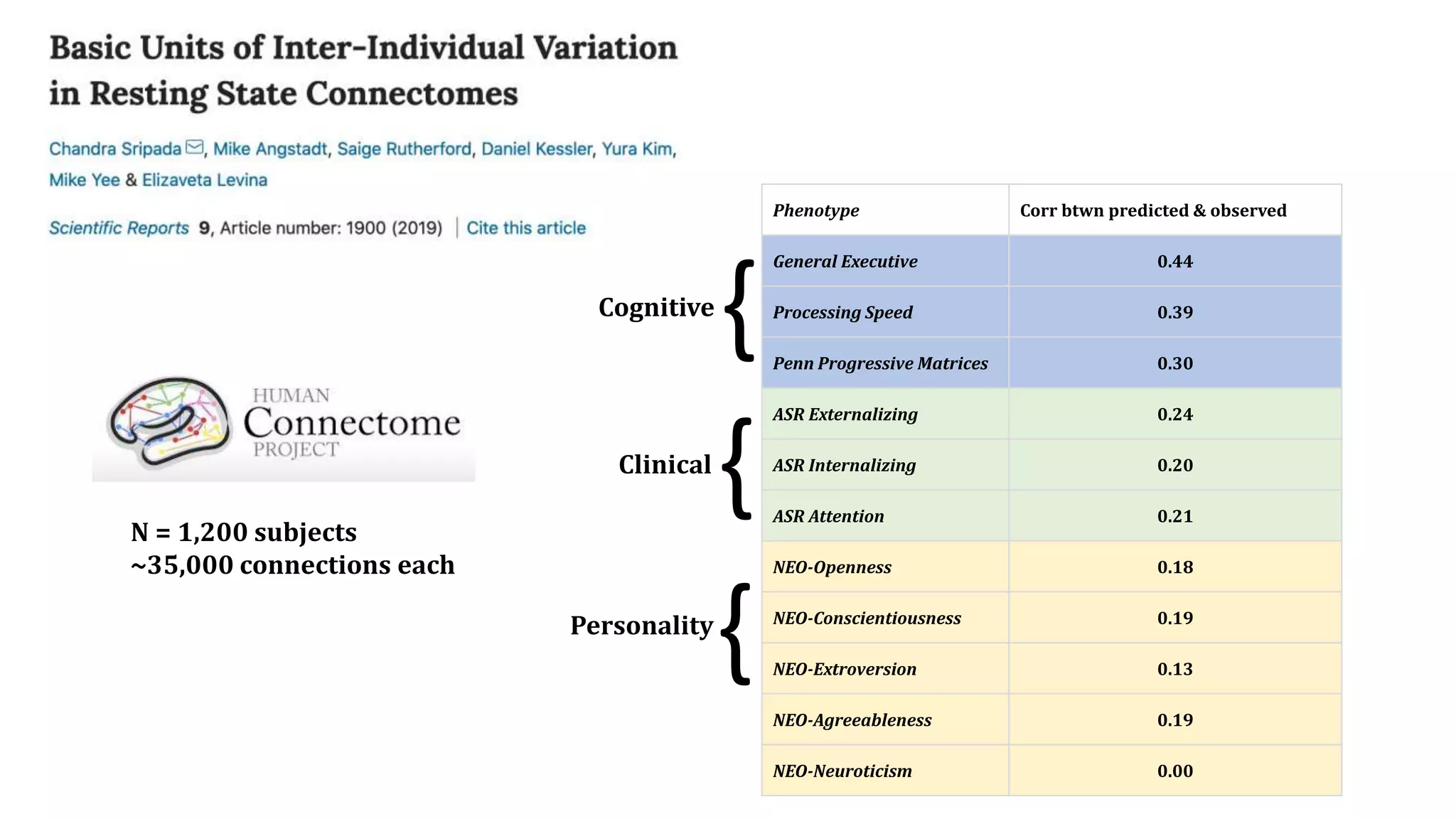
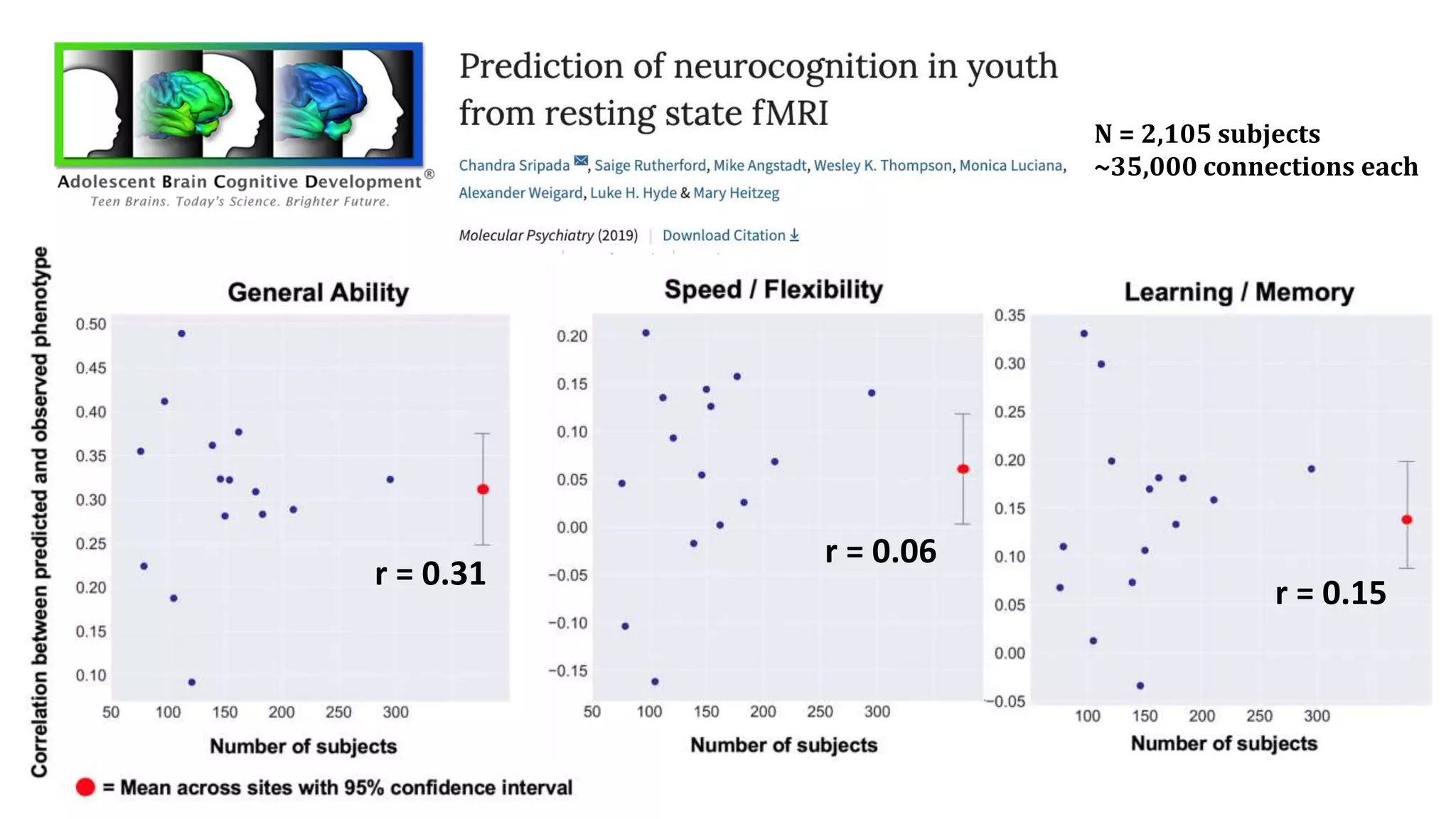
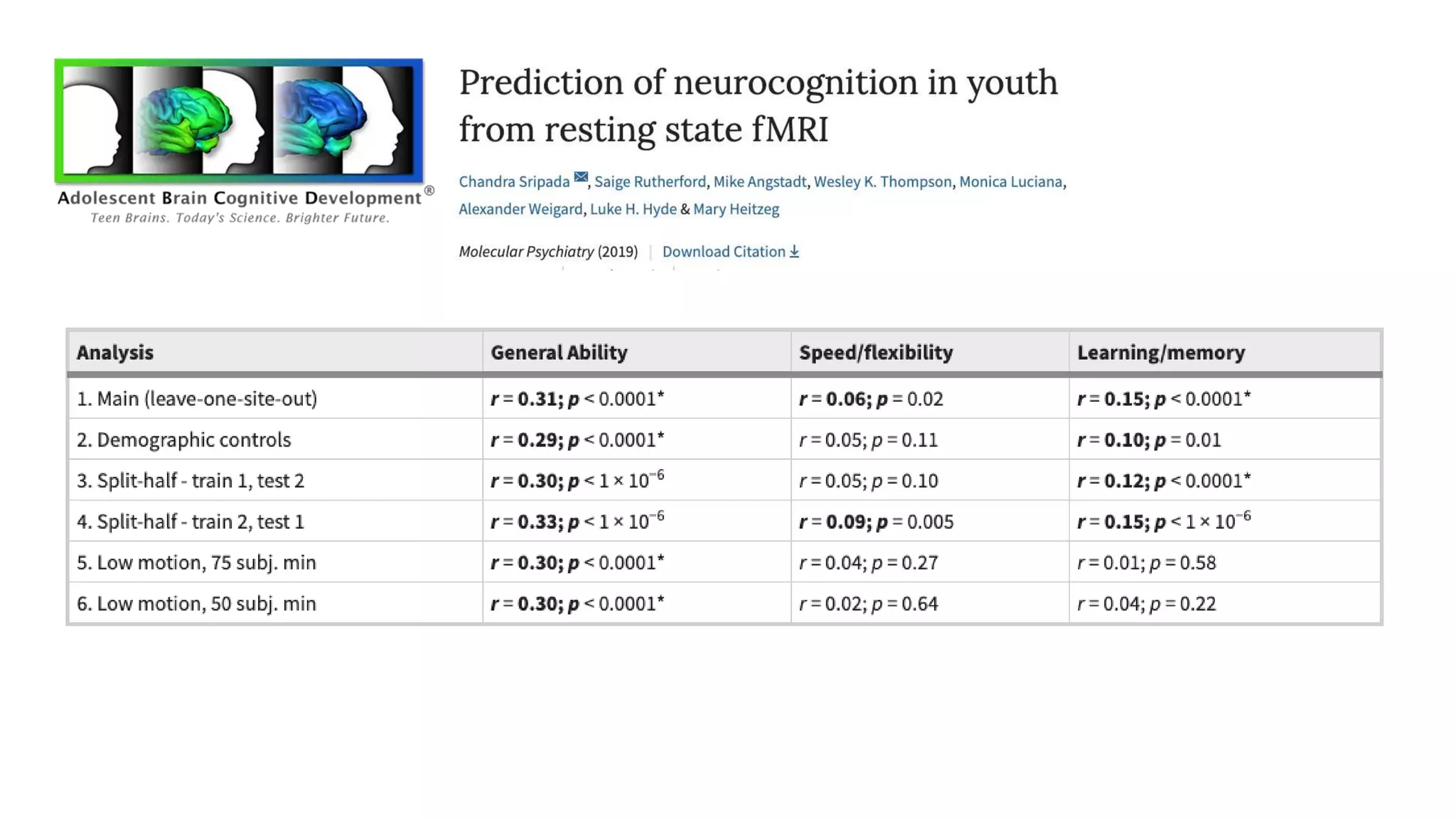
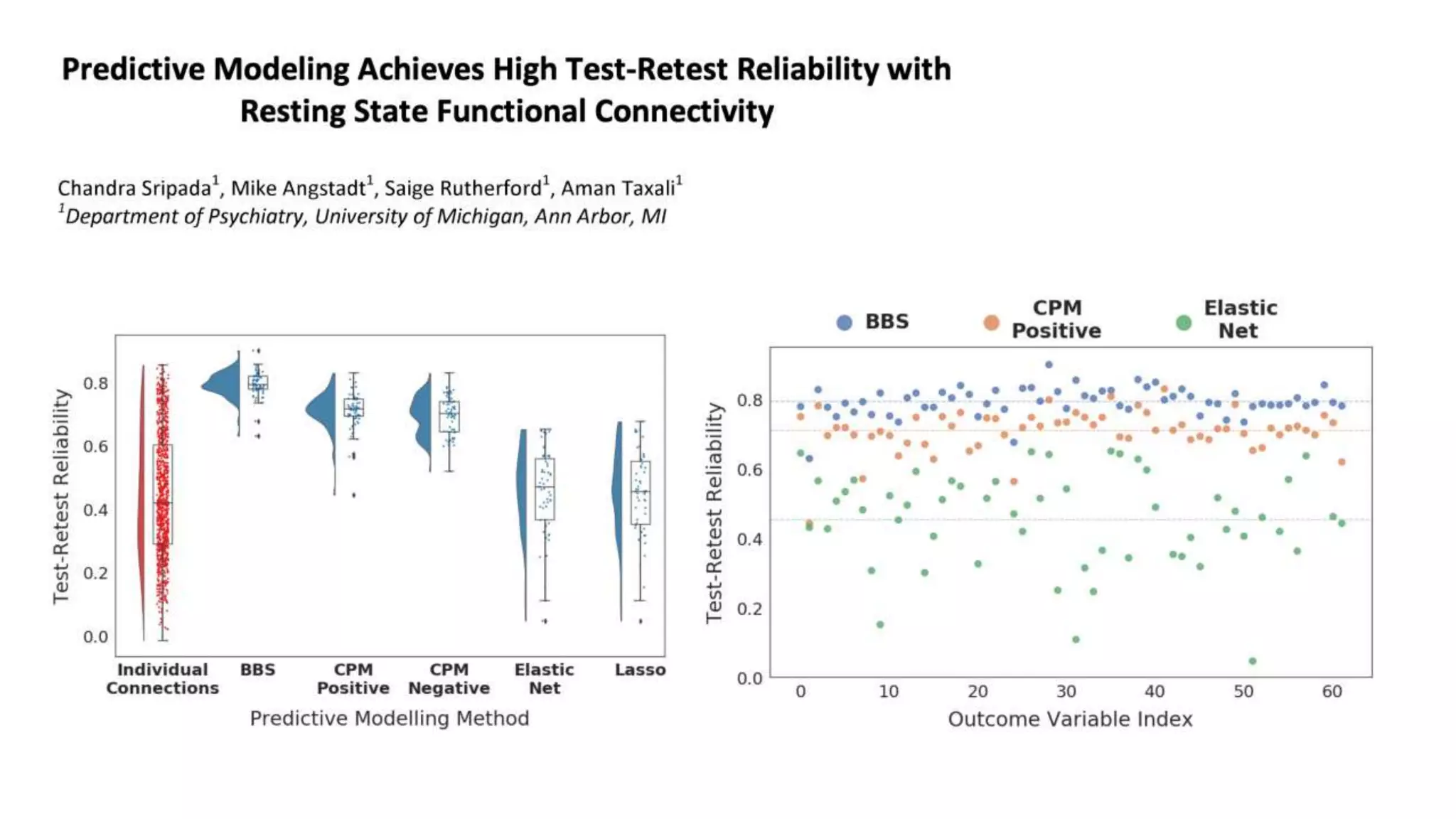
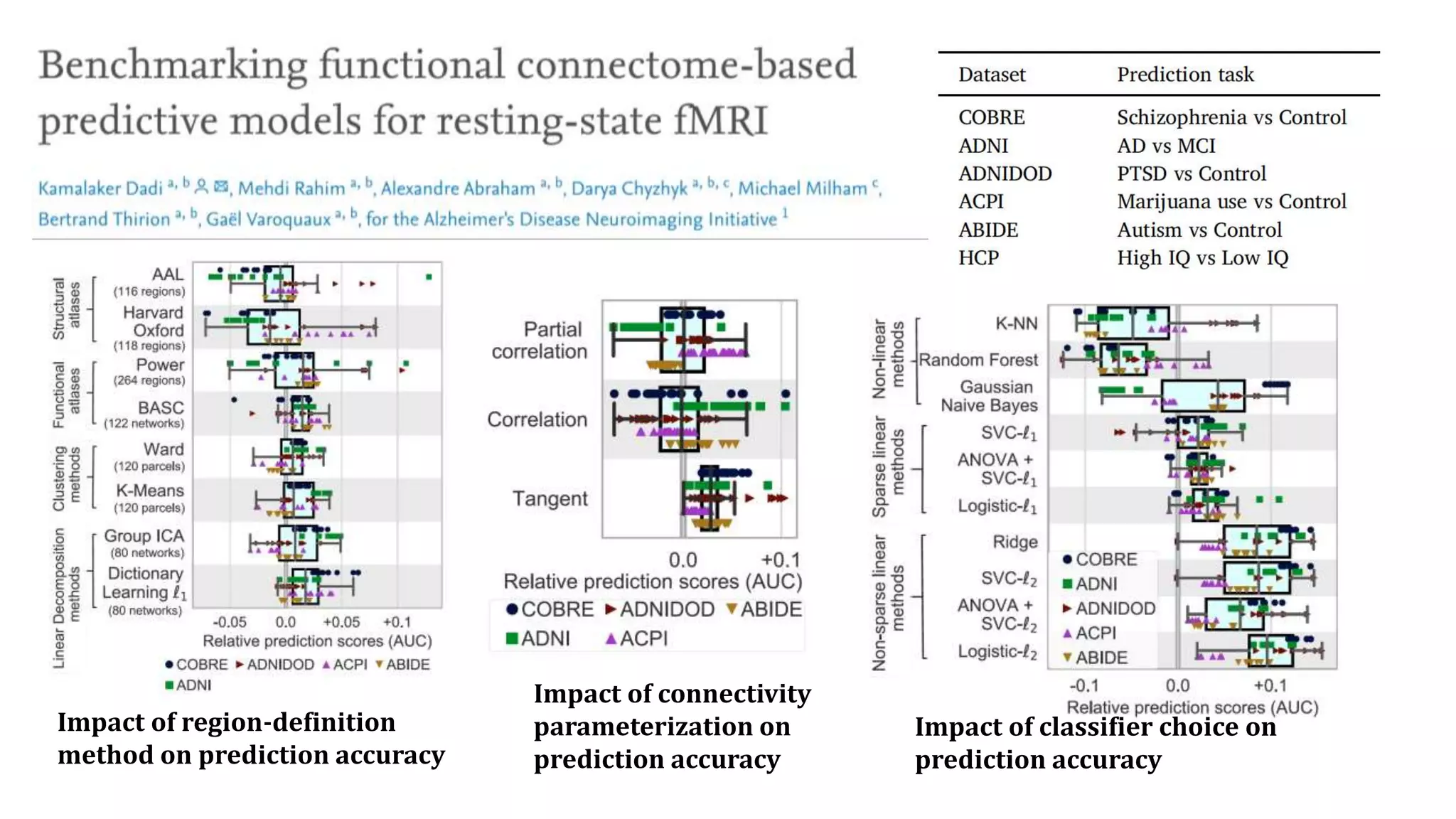
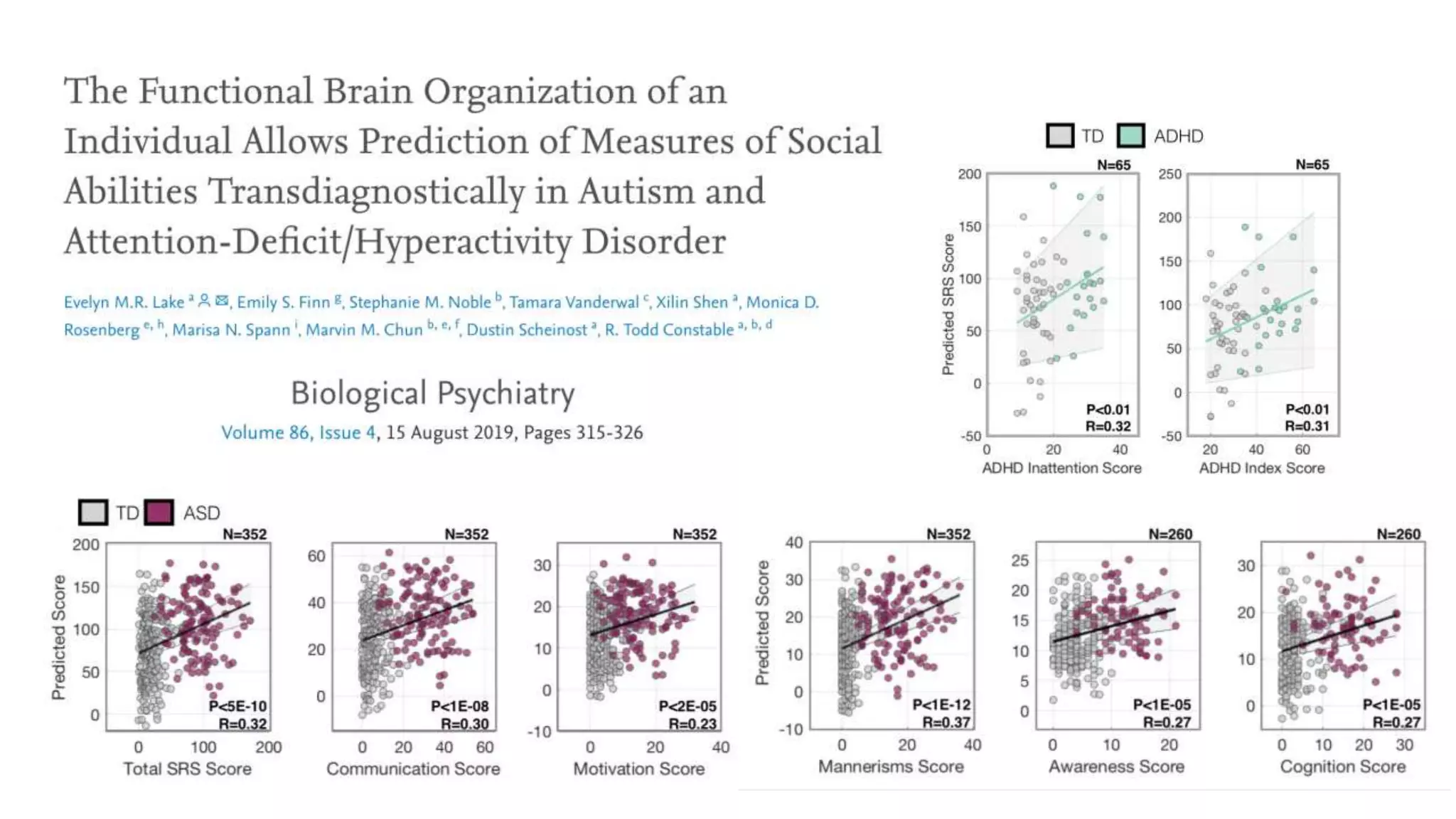
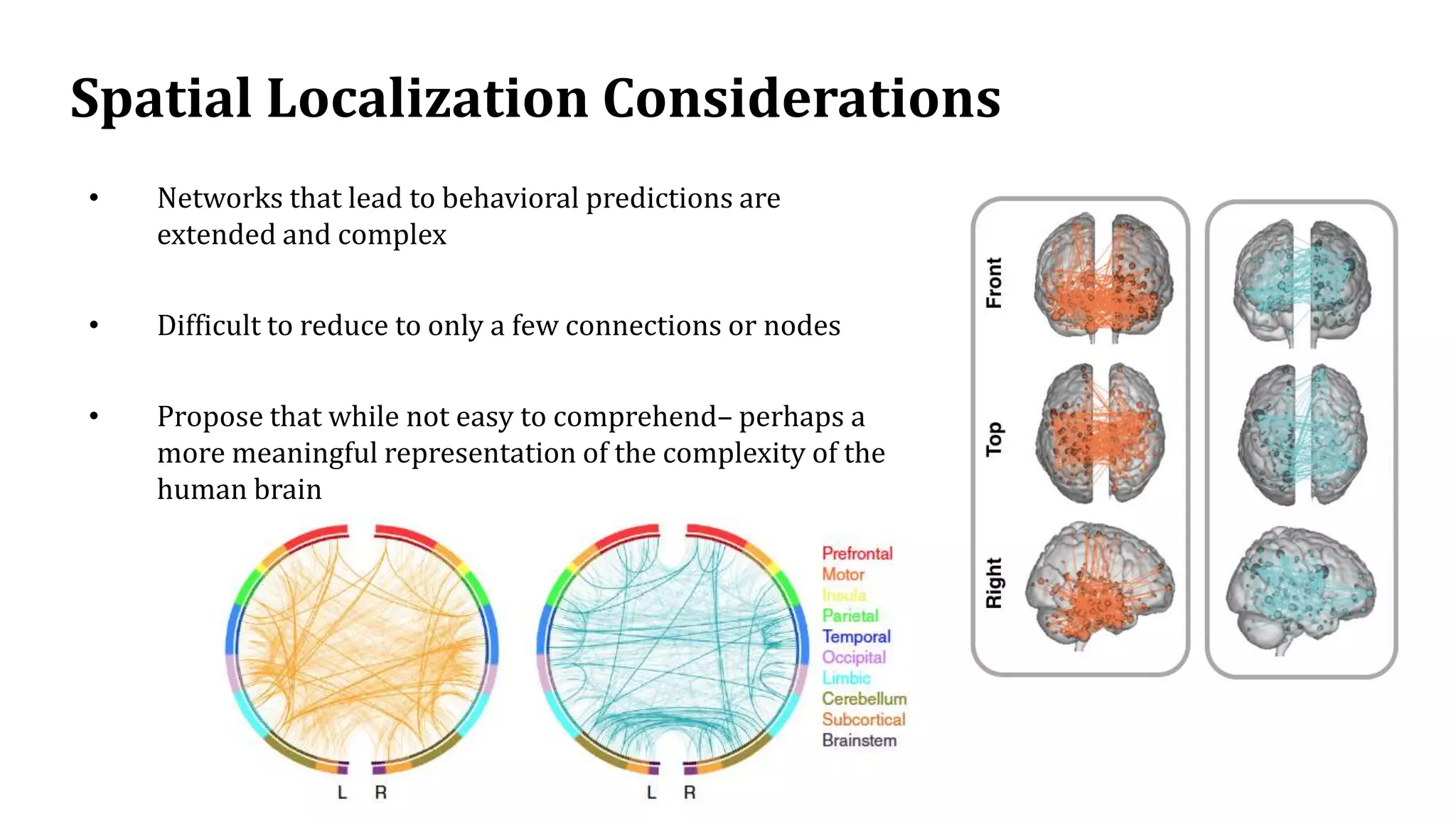
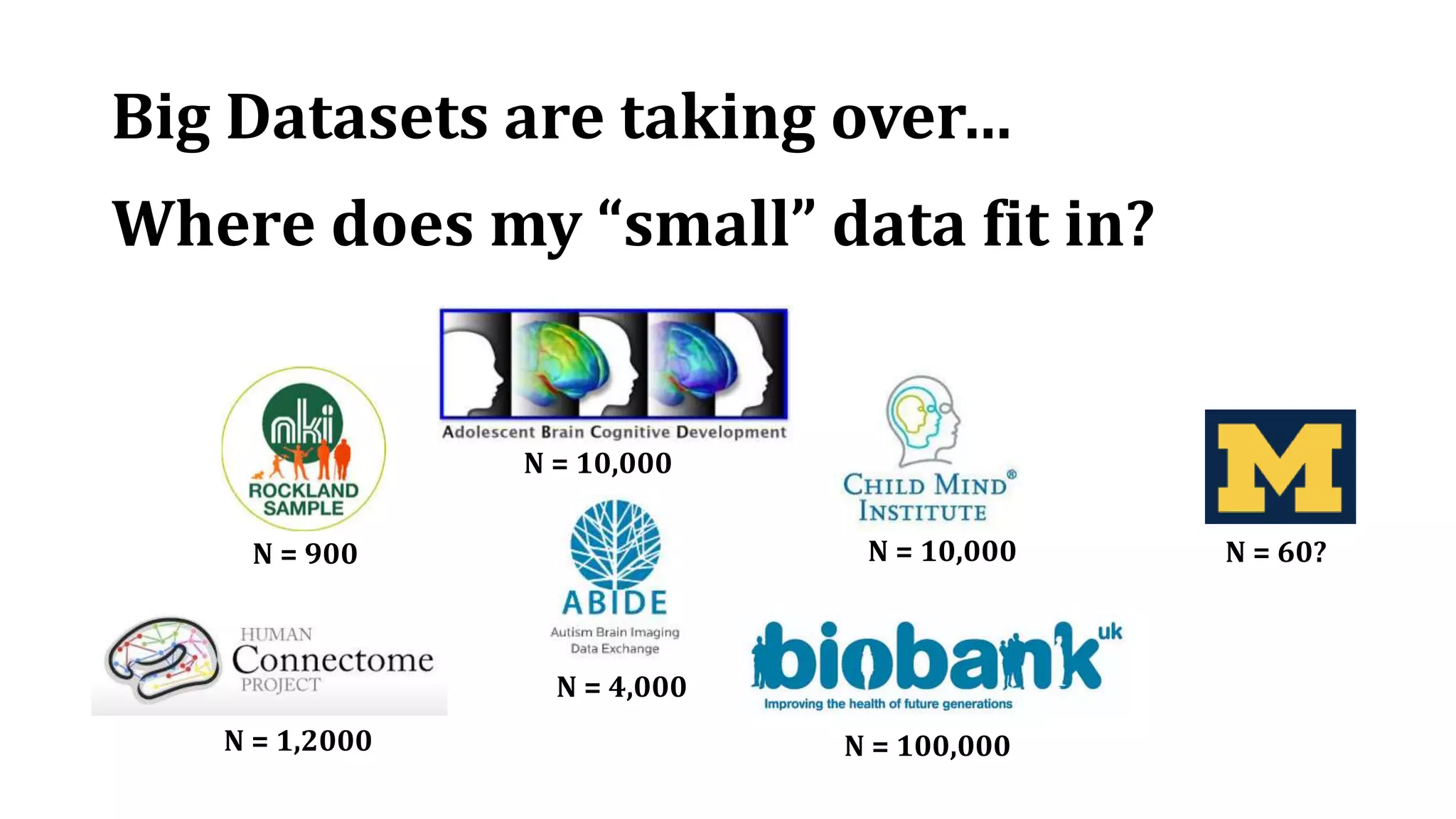
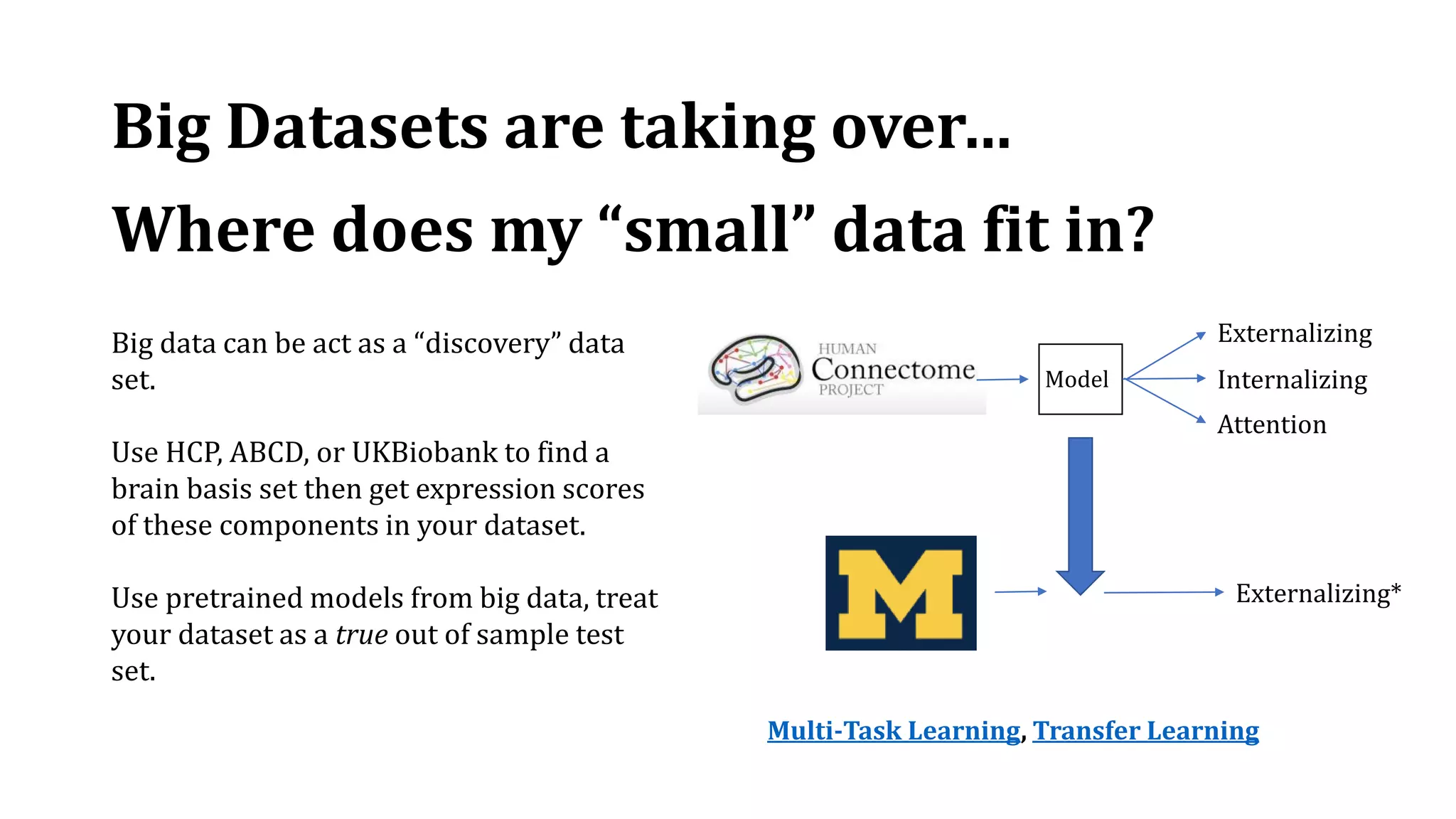
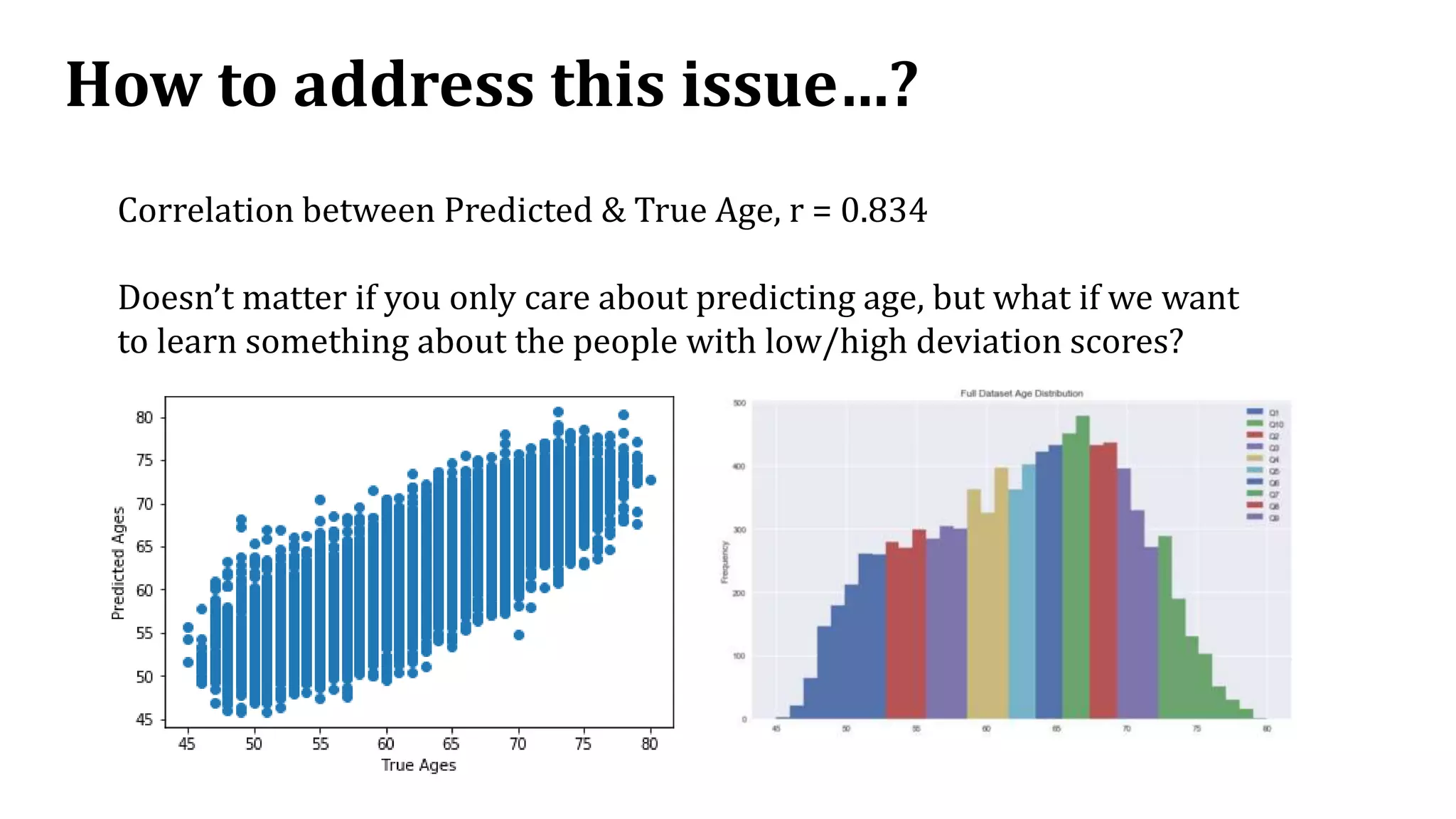
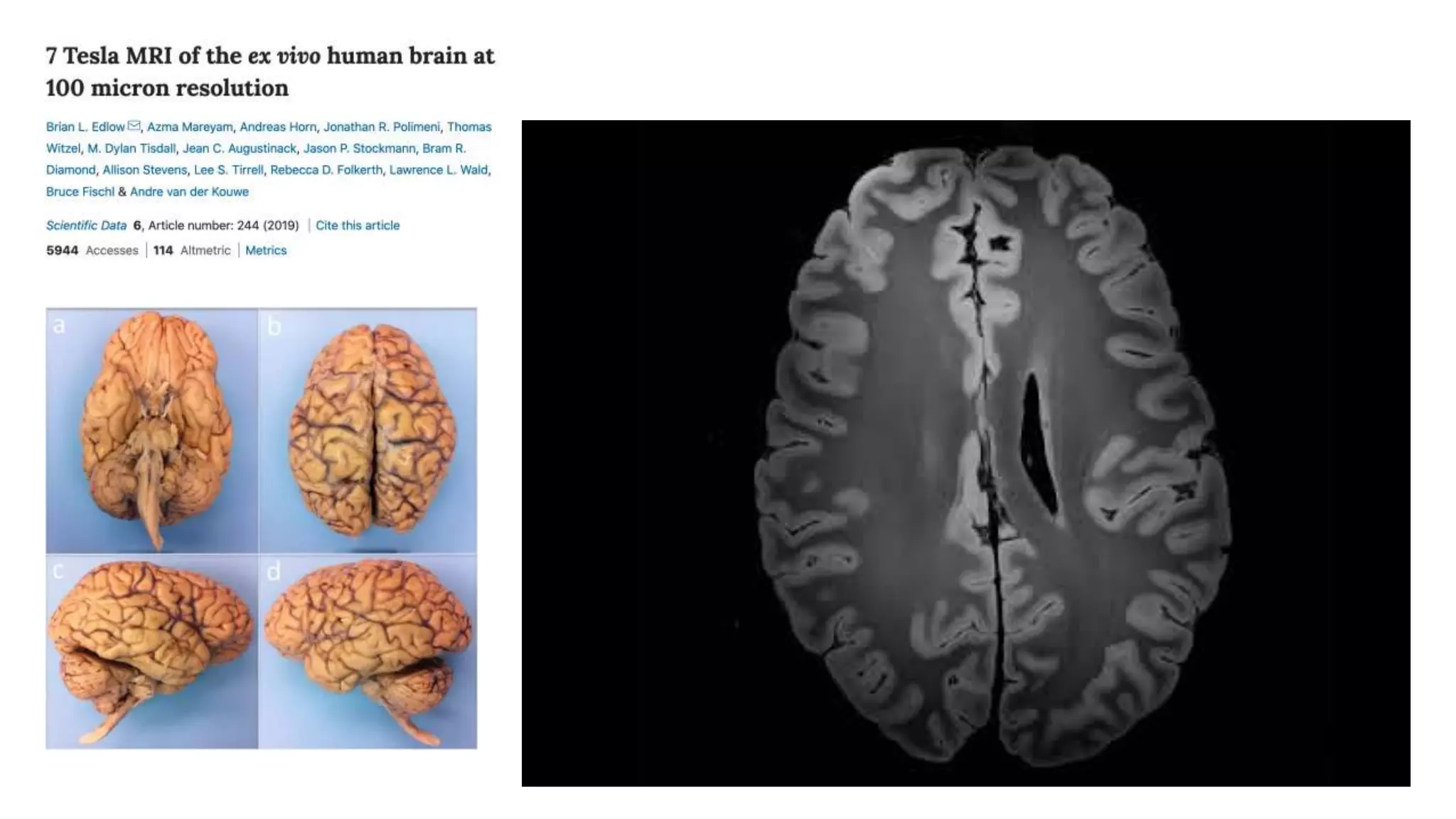
This document summarizes a presentation on predicting traits and behaviors from neuroimaging data. It provides an overview of neuroimaging techniques like MRI and fMRI, how brain connectivity networks are analyzed, and methods for predictive modeling of behaviors from brain images. The presentation shows it is possible to reliably predict some cognitive traits and phenotypes from whole-brain connectivity patterns, with the highest correlations being for general executive function, processing speed, and cognitive test scores. It discusses challenges like interpretation of predictive models and limitations of small clinical datasets. The talk advocates moving away from categorical diagnoses toward dimensional assessment of symptom spectra and acknowledges limitations in neuroimaging data related to bias.