Download to read offline


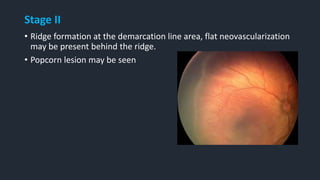
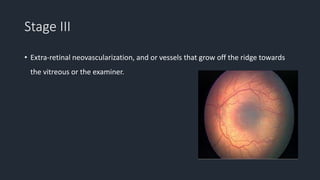
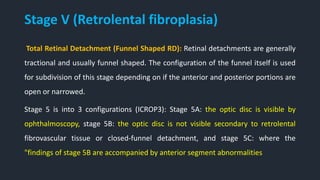
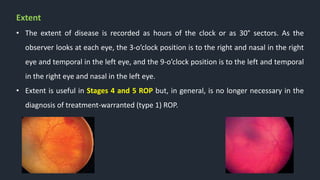



This document provides information on Retinopathy of Prematurity (ROP), including its history, risk factors, pathophysiology, screening guidelines, physical exam findings, classification system, management, and termination of screening criteria. ROP is a serious eye disorder in premature infants that can lead to blindness. It results from disrupted retinal vascular development due to premature birth. The smallest and sickest preterm infants have the highest risk. Screening is important and involves examination to stage the ROP based on location and severity. Management may include frequent follow-up exams or treatment depending on ROP stage.































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















