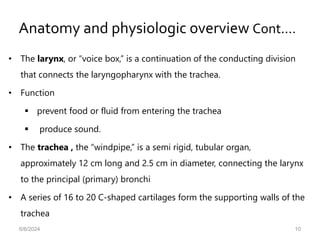
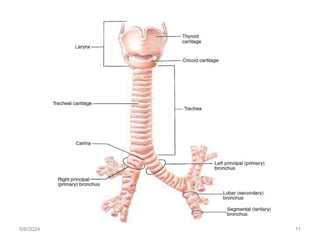
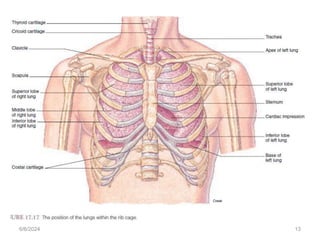
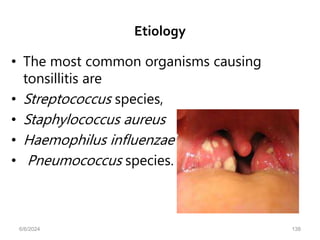
The document provides a comprehensive overview of medical-surgical nursing management for patients with respiratory disorders, focusing on anatomy, assessment, and examination techniques. Key lesson objectives include revising respiratory anatomy, performing health history assessments, demonstrating physical examinations, and identifying diagnostic procedures. The text covers the anatomy of the respiratory system, its functions, examination methods, and common symptoms related to respiratory issues.





![• H. influenzae is another cause of CAP.
• It frequently affects elderly people or those with comorbid
illnesses (eg, chronic obstructive pulmonary disease
[COPD], alcoholism, diabetes mellitus).
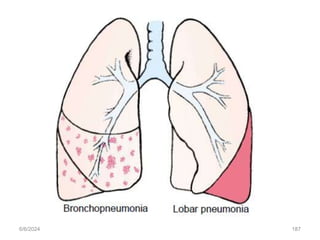
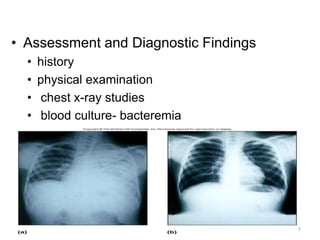
• Chest x-rays may reveal multilobar, patchy
bronchopneumonia or areas of consolidation
6/6/2024 189](https://image.slidesharecdn.com/rispiratorydisordersfornurses-240606061836-3d4f226f/85/rispiratory-disorders-for-nurses-pptxbb-188-320.jpg)

![• Use controlled coughing .
• Keep secretions liquid.
– Encourage high level of fluid intake (8 to 10 glasses; 2 to 2.5 L] daily)
within level of cardiac reserve.
– Give continuous aerolized sterile water or nebulized normal saline to
humidify bronchial tree and liquefy sputum if appropriate.
– Avoid dairy products if these increase sputum production.
6/6/2024 309](https://image.slidesharecdn.com/rispiratorydisordersfornurses-240606061836-3d4f226f/85/rispiratory-disorders-for-nurses-pptxbb-307-320.jpg)