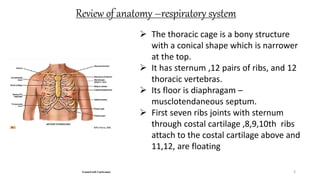
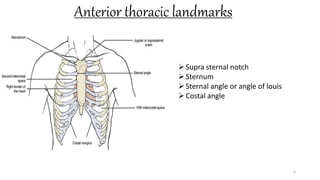
This document provides information on conducting a respiratory assessment. It begins with an introduction on obtaining an accurate health history and physical exam. It then reviews anatomy of the respiratory system and key landmarks. The document outlines components of a respiratory assessment including demographic data, chief complaints, review of systems, past medical history, medications, and physical exam techniques. The physical exam section describes inspection of the nose, mouth, neck, chest, and auscultation.







































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)












