Download as PDF, PPTX
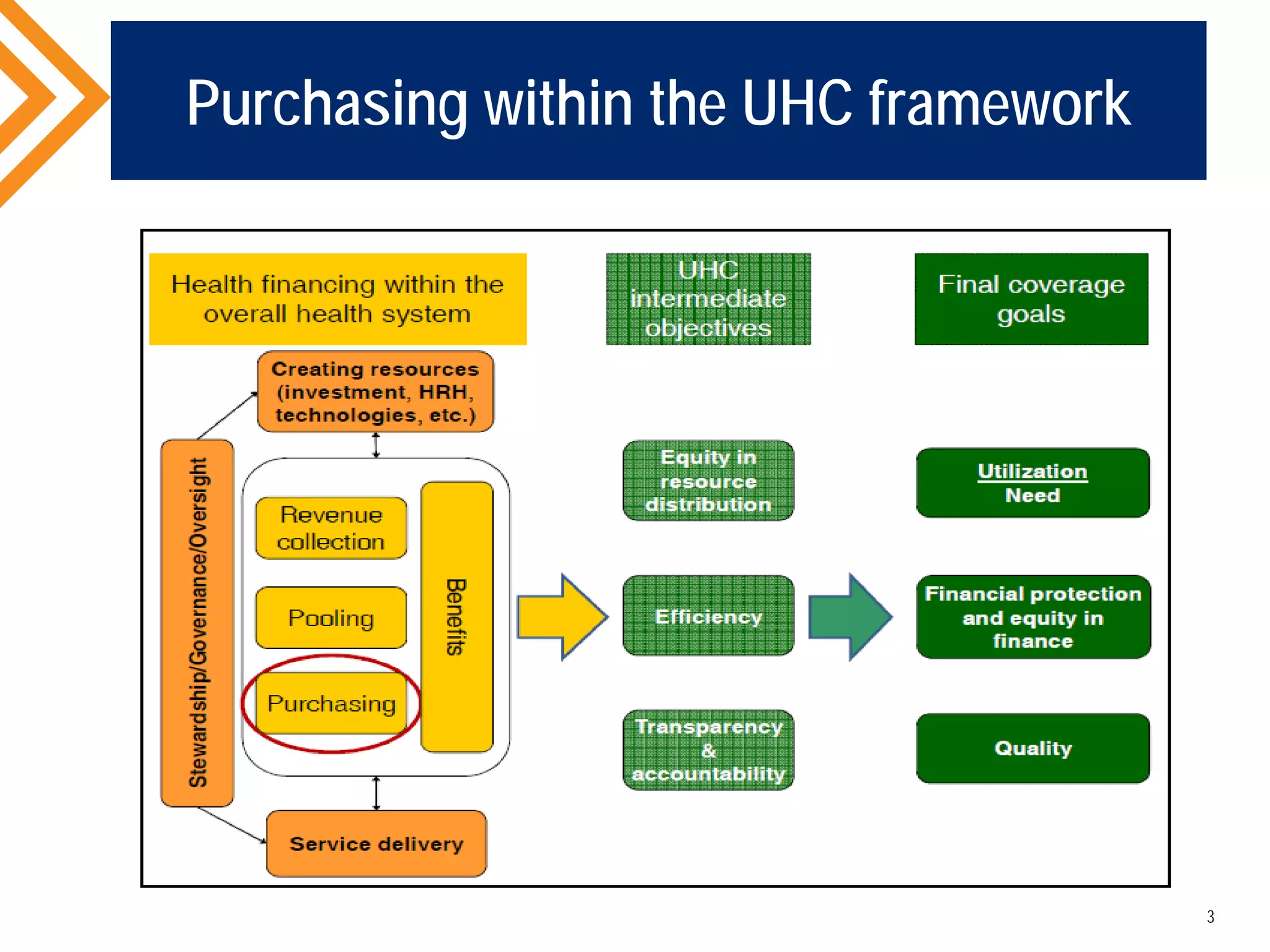
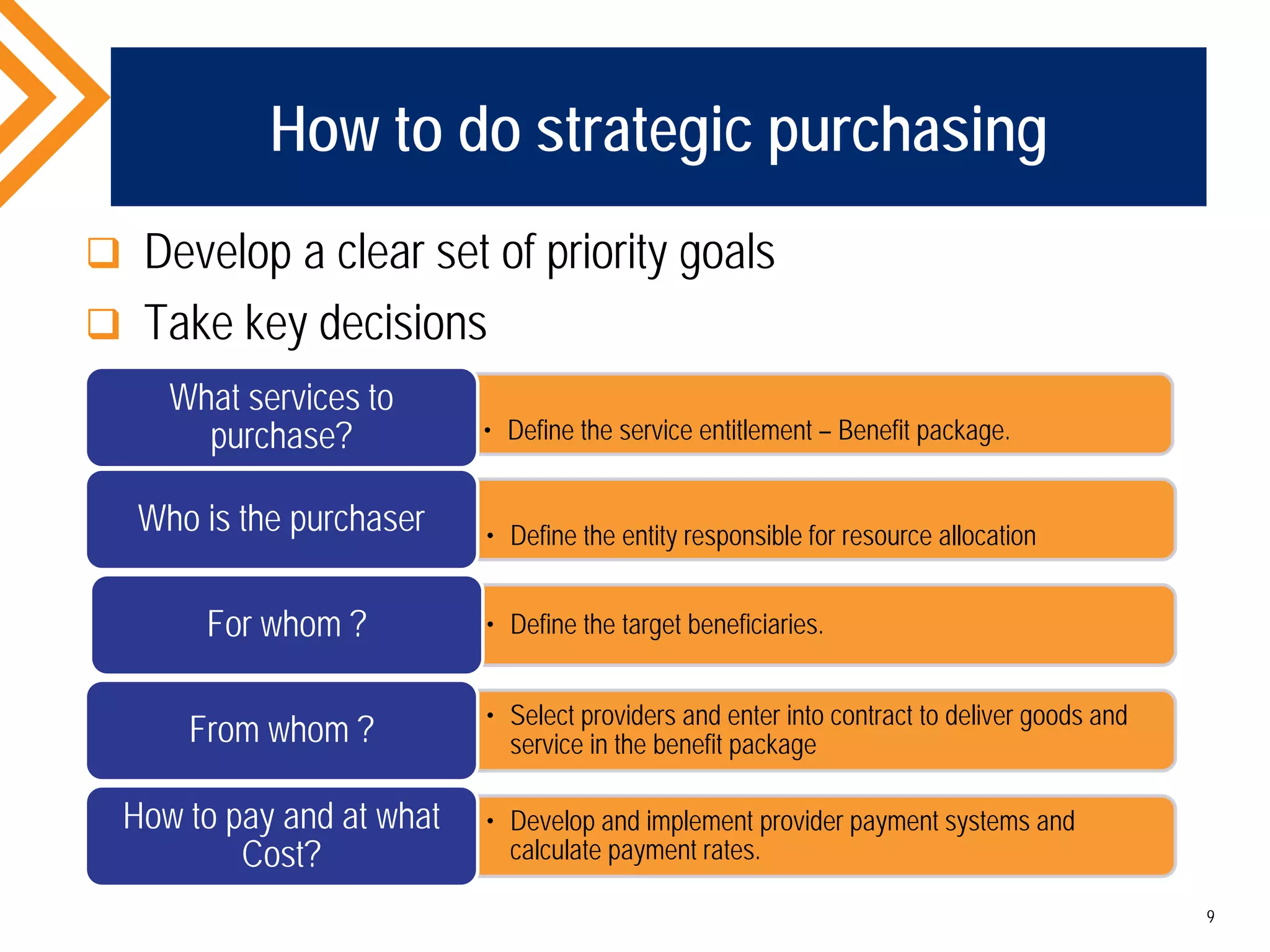


The document discusses the significance of strategic purchasing in health systems, emphasizing its role within the universal health coverage (UHC) framework. It outlines the differences between purchasing and procurement, the importance of aligning purchasing with health objectives, and how strategic purchasing can improve efficiency, equity, and the quality of health services. Key steps in implementing strategic purchasing include defining goals, selecting service providers, and utilizing effective governance and technology.



















































































