Download to read offline




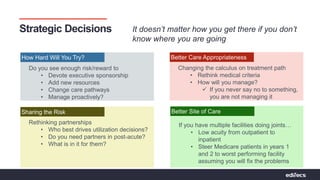
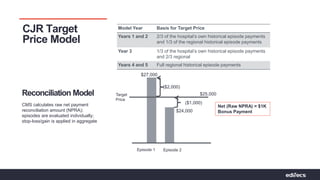
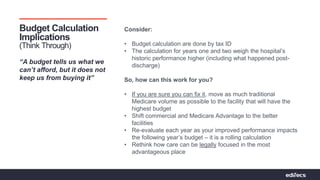

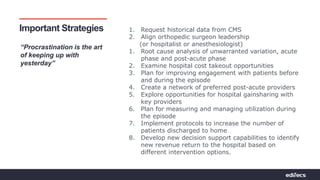
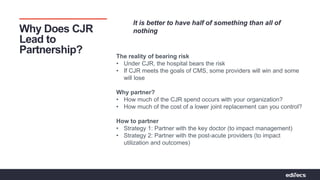

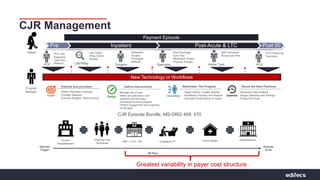


The document outlines strategies for hospitals to successfully navigate the Comprehensive Joint Replacement (CJR) model, emphasizing the importance of partnerships and strategic decision-making to manage care and costs effectively. It highlights the need for hospitals to bear the financial risk while improving patient engagement, care pathways, and aligning with post-acute providers. Essential strategies include historical data analysis, enhancing physician collaboration, and utilizing technology for better performance management throughout the care episode.











































































