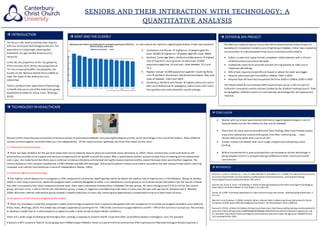
This document discusses research on seniors' use of technology for out-of-hospital care. It summarizes three key studies: 1) online communities can benefit seniors' well-being, 2) internet-based interventions reduced stress in caregivers versus controls, and 3) a technology acceptance model predicted seniors' use of assistive social agents. It also notes the increasing elderly population in the UK and their burden on the health system. Statistics on Kent County show areas with the highest elderly populations and rates of nursing home residence and home care use.