Functions of Kidney
Maintenance of extracellular fluid volume &
composition
Excretion of metabolic waste products
Regulation of blood pressure by renin angiotensin
mechanism.
Synthesis of erythropoietin
Production of vit.D3 (active form)
3.
Indications
Early identificationof impairment of renal function in
patients with increased risk of chronic renal disease
Diagnosis of renal disease
Follow the course of renal disease and assess response to
treatment
Plan renal replacement therapy (dialysis or renal
transplantation) in advanced renal disease
Adjust dosage of certain drugs (eg. Chemotherapy)
according to renal function.
Tests to EvaluateGlomerular Function
Normal GFR : 120-130ml/min per 1.73 sq.m
Declines progressively at the rate of 1
ml/minute/year after 40 years of age
6.
Clearance Tests toMeasure Glomerular Filtration
Rate
If a substance is not bound to protein in plasma, is
completely filtered by the glomeruli, and is neither
secreted nor reabsorbed by the tubules, then its
clearance rate is equal to glomerular filtration rate.
Clearance=UV/P
U=concentration of a substance in urine in mg/dl
V=volume of urine excreted in ml/min
P=concentration of the substance in plasma in mg/dl
7.
Inulin clearance
Clearance of Radiolabeled Agents
Cystatin C clearance
Creatinine clearance
Urea clearance
8.
Inulin Clearance
Inulinis an inert plant polysaccharide, is filtered by
glomeruli & is neither reabsorbed nor secreted by the
tubules.
A bolus dose (25 ml of 10% IV)is administered followed
by constant IV infusion (500ml of 1.5% soln at the rate of
4ml/min)
Timed urine samples are collected & blood samples are
obtained at the midpoint of timed urine collection.
Normal inulin clearance for males:90-139ml/min/1.73sqm
Normal inulin clearance for females:80-125ml/min/1.73sqm
9.
Clearance ofradiolabeled agents: 51Cr-EDTA &
99Tc-DTPA
Cystatin C clearance:
cystine protease inhibitor is produced by all
nucleated cells at constant rate.
Its level is not affected by sex, diet or muscle
mass.
It is measured by immunoassay.
10.
Creatinine clearance:
completelyfiltered by glomeruli & not
reabsorbed by tubules.
A 24 hr urine sample is preferred to overcome
problems of diurnal variation.
It is derived from formula C=UV/P
Men :110-150 ml/min/1.73 sqm
Women : 105-132 ml/min/1.73 sqm
11.
Urea clearance
Urea is filtered by the glomeruli, but about 40% of the filtered
amount is reabsorbed by the tubules.
The reabsorbtion depends on the rate of urine flow.
Thus, it underestimates GFR, depends on the urine flow rate &
not a sensitive indicator of GFR.
12.
Estimation of CreatinineClearance from Serum
Creatinine by Prediction Equations
Creatinine clearance in ml/min =
(140-Age in years) x (Body weight in kgs)/
(72 x Serum creatinine in mg/dl)
In females, the value obtained from above equation is multiplied
by 0.85 to get the result.
Causes ofincreased BUN:
1) Pre renal azotemia : shock, ccf, water & salt deprivation
2) Renal azotemia: impairment of renal function
3) Post renal azotemia : urinary tract obstruction
4) Increased rate of production of urea:
High protein diet
Increased protein catabolism (trauma, burns, fever)
Absorbtion of amino acids & peptides from large haemorrhage in
GIT
Causes ofincreased serum creatinine :
1. Pre renal, renal & post renal azotemia
2.Large amount of dietary meat
3.Active acromegaly & giagantism
17.
Blood Biochemistry
BUN/SerumCreatinine Ratio :
Normal range : 12:1 to 20:1
Causes of increased BUN/Creatinine ratio (>20:1)
Increased BUN with normal serum creatinine
Pre renal azotemia
High protein diet
Increased protein catabolism
Increase of both BUN & serum creatinine with disproportionately
greater increase of BUN:
Post renal azotemia
Obstruction to the urine outflow causes diffusion of urinary
urea back into the blood from tubules because of back pressure
18.
Microalbuminuria and Albuminuria
Microalbuminuria :30-300mg/24hrs
Overt albuminuria : >300mg/24hrs
Microalbinuria is the earliest evidence of
glomerular damage in DM
19.
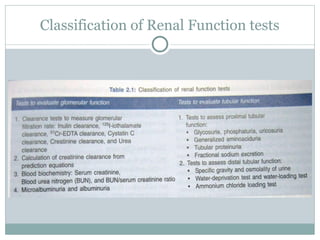
Tests to EvaluateTubular Function
Tests to Assess Proximal Tubular Function
Glycosuria
Generalised aminoaciduria
Tubular proteinuria
Urinary concentration of sodium
Functional excretion of sodium
[( Urine sodium x plasma creatinine)/(plasma sodium x urine
creatinine)] x 100
20.
Tests toAssess Distal Tubular Function
Urine specific gravity
Urine osmolality
Water deprivation test
Water loading anti diuretic hormone suppression test
Ammonium chloride loading test ( Acid load test)
21.
Tests toAssess Distal Tubular Function
Urine specific gravity- ratio of mass of solution to the mass of
water
SG is a measure of concentrating ability of kidneys.
Urinometer method :
Principle of buoyancy i.e. the ability of the fluid to exert
an upward thrust on a body placed in it.
normal value : 1.003-1.030
Increased in DM, Nephrotic syndrome & dehydration
Decreased in diabetes insipidus, CRF & compulsive water
drinking
22.
Tests toAssess Distal Tubular Function
Urine osmolality –number of dissolved particles in a solution
Urine/plasma osmolality ratio is helpful in
distinguishing pre renal azotemia (in which ratio is
higher) from acute renal failure due to acute tubular
necrosis (ratio is lower)
23.
Tests toAssess Distal Tubular Function
Water deprivation test
Water intake is restricted for a specified time followed by
measurement of specific gravity or osmolality .
Normally, urine osmolality should rise in response to water
deprivation.
If it fails to rise, then desmopressin is administered.
Urinary concentrating ability is corrected after
administration of desmopressin in central diabetes insipidus, but
not in nephrogenic type.
24.
Tests toAssess Distal Tubular Function
Water loading anti diuretic hormone suppression test
After overnight fast, patient empties the bladder & drinks 20 ml/kg water
in 15-20 minutes.
Urine is collected at hourly intervals for next 4 hours for measurements of
urine volume, sp. Gravity & osmolality.
Plasma levels of ADH & serum osmolality should be measured at hourly
interval.
Normally >90% water should be excreted in 4hrs.
Specific gravity should fall to 1.003 & osmolality <100 mOsm/kg
If renal function is impaired, urine volume is reduced & sp. gravity &
osmolality fail to decrease.
25.
Tests toAssess Distal Tubular Function
Ammonium chloride loading test ( Acid load test)
Urine pH & plasma HCO3 levels are measured after overnight fasting.
If pH is < 5.4 , acidifying ability of renal tubules is normal.
If pH is >5.4 & plasma HCO3 is low, diagnosis of renal tubular acidosis
is confirmed.
To confirm further patient is given ammonium chloride (0.1m/kg) over
1 hour after overnight fast & urine samples are collected hourly for next 6-8 hrs.
ammonium ions dissociate into H & NH3 & makes blood acidic.
thus, if pH is <5.4 acidifying ability of the distal tubule is normal.
26.
Renal Biopsy
Indications forRenal Biopsy
Nephrotic syndrome in adults
Nephrotic syndrome not responding to corticosteroids in children
Acute nephritic syndrome for differential diagnosis
Unexplained renal insufficiency with near-normal kidney dimensions on
ultrasonography
Asymptomatic hematuria, when other diagnostic tests fail to identify the source of
Bleeding
Isolated non-nephrotic range proteinuria (1-3gm/24hrs) with renal impairment
Impaired function of renal graft
Involvement of kidney in systemic lupus erythematous or amyloidosis
27.
Contraindications
Uncontrolled severehypertension
Hemorrhagic diathesis
Solitary kidney
Renal neoplasm (to avoid spread of malignant cells along the needle track)
Large and multiple renal cysts
Small, shrunken kidneys
Acute urinary tract infection like pyelonephritis
Urinary tract obstruction



![Tests to Evaluate Tubular Function
Tests to Assess Proximal Tubular Function
Glycosuria
Generalised aminoaciduria
Tubular proteinuria
Urinary concentration of sodium
Functional excretion of sodium
[( Urine sodium x plasma creatinine)/(plasma sodium x urine
creatinine)] x 100](https://image.slidesharecdn.com/renalfunctiontests-251229165413-2286a1a4/85/Renal_Function_tests-Renal-health-assessment-ppt-19-320.jpg)





































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














