z
HOMEOS
Homeostasis isthe ability of a biological system to m
stable internal environment despite external changes
optimal conditions for cellular function by regulating v
such as temperature, pH, electrolyte balance, and flu
z
ROLE OF K
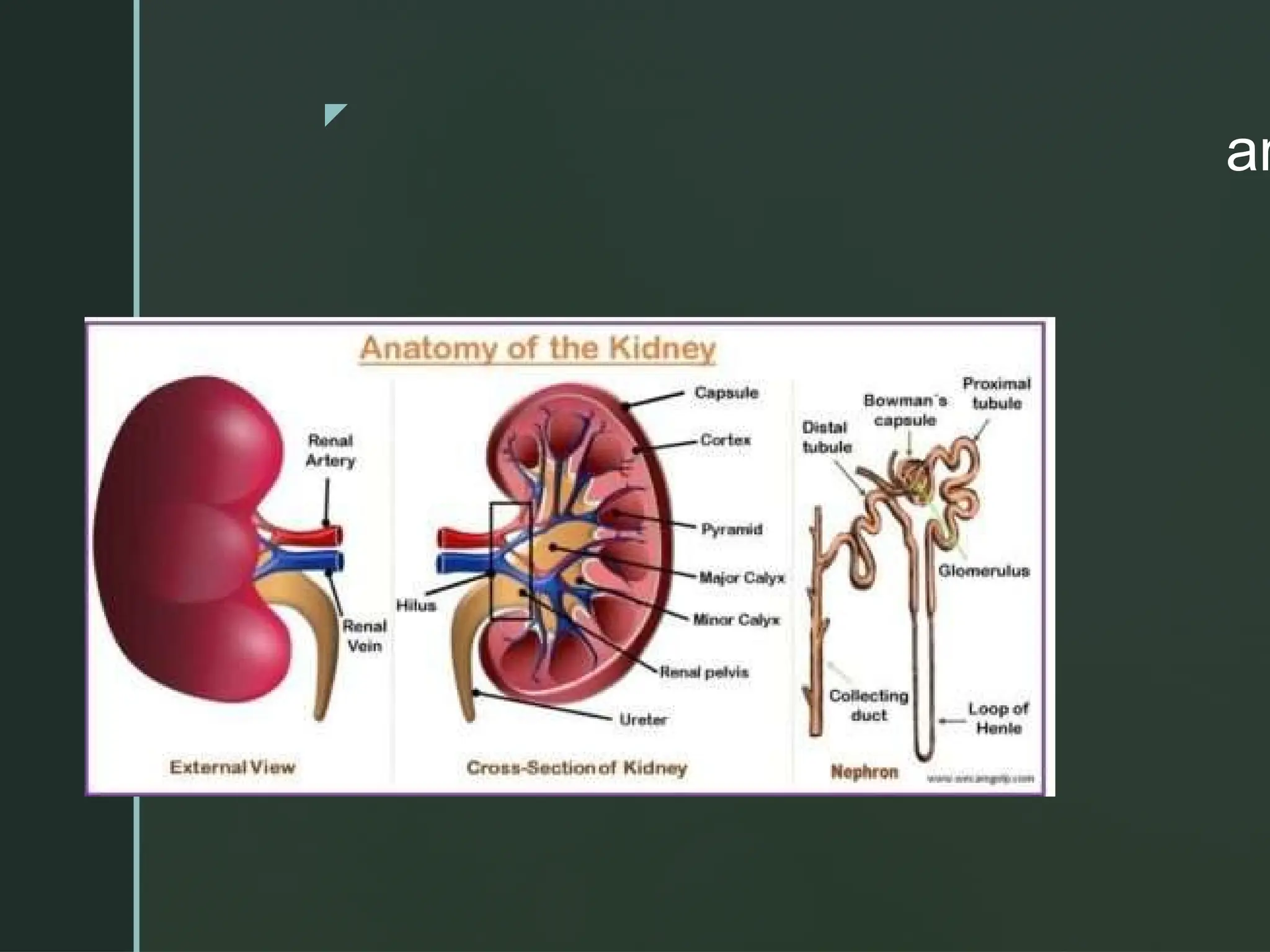
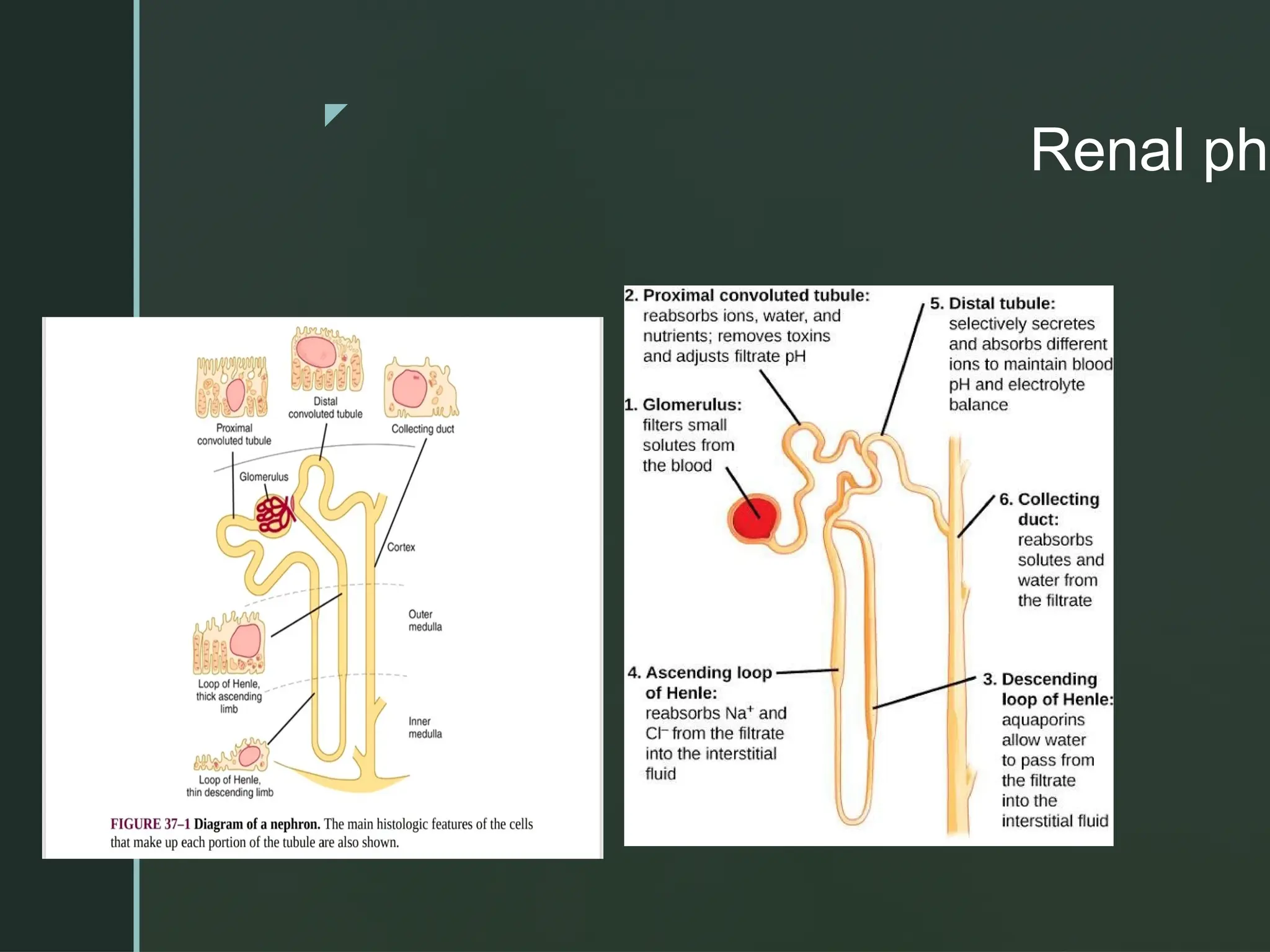
OVERVIEW OF KIDNEY
The kidney play a crucial role in filtering blood,balanc
electrolytes,regulating blood pressure,and excreting w
products
z
Renal phys
Fluidand Electrolyte Balance – Regulating water, sodium, potassium
electrolytes.
Acid-Base Balance – Maintaining blood pH.
Waste Removal – Excreting metabolic waste and toxins.
Blood Pressure Regulation – Modulating blood volume and pressure
Erythropoiesis – Stimulating red blood cell production in response to
Bone Health – Managing calcium and phosphate levels.
Detoxification – Eliminating harmful substances from the body. The k
vital organs that maintain internal stability through their regulatory fun
7.
z
Acid-base b
MaintainingpH
Kidney plays an important role in maintenance of acid-
base balance by excreting hydrogen ions and retainingbicarbonate ions.
Normally, urine is acidic in nature with a pH of 4.5 to6.
Metabolic activities in the body produce large quantity of acids (with lot o
ions), which threatento push the body towards acidosis.
However, kidneys prevent this.
Kidneys prevent acidosis by two ways:
1. Reabsorption of bicarbonate ions (HCO3)
2. Secretion of hydrogen ions (H+).
8.
z
Role of kidneyin homeo
The kidneys are crucial in maintaining homeostasis, w
body's ability to maintain stable internal conditions de
external changes. The kidneys regulate several phys
parameters to ensure the internal environment remain
for cell function.
9.
z
Renal Hor
Erythropoietin(EPO)
Renin (Part of the Renin-Angiotensin-Aldosterone Sy
RAAS)
Calcitriol (Active Vitamin D)
10.
z
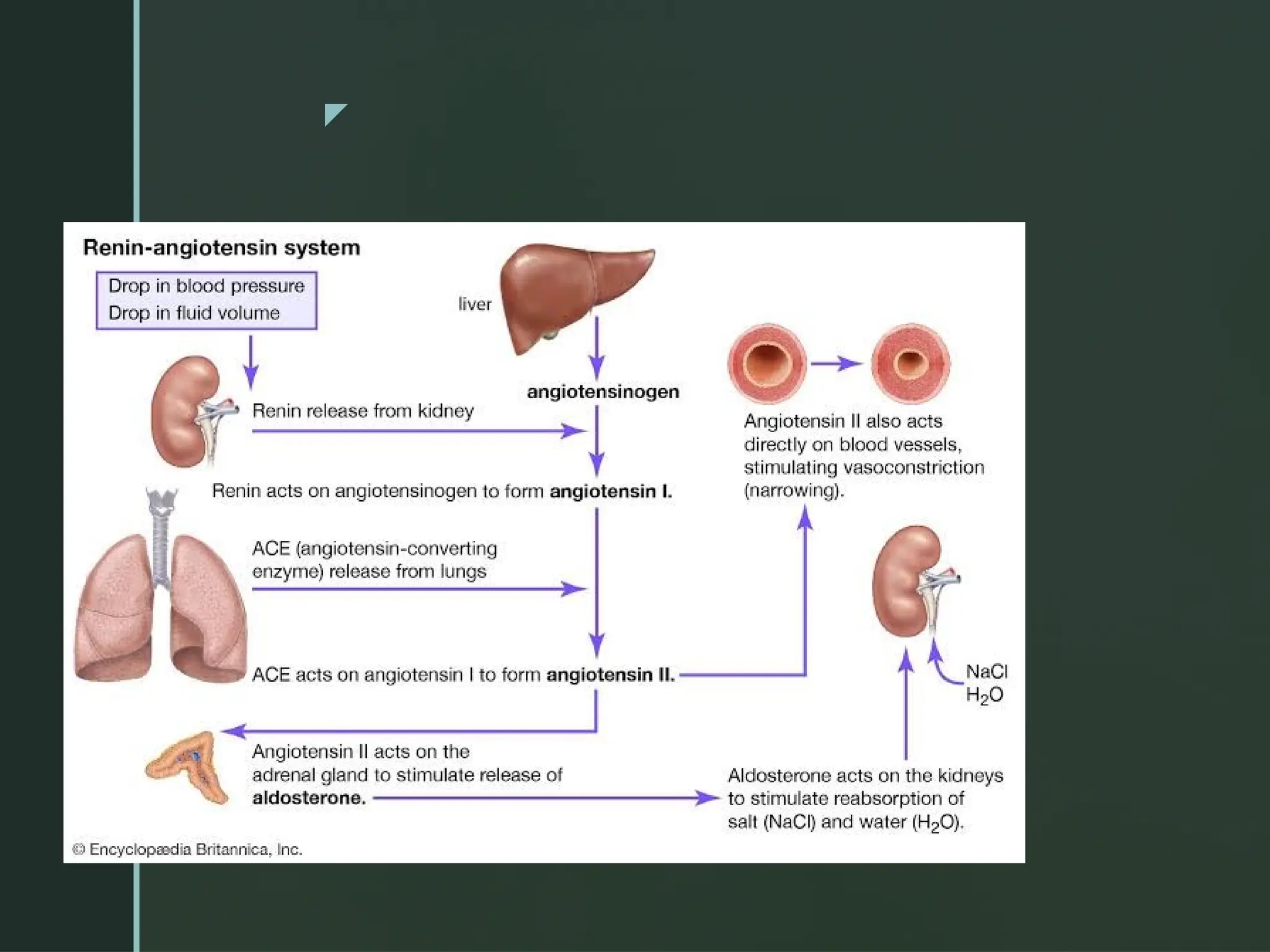
Renin (Partof the Renin-Angiotensin-Aldosterone System, RAAS).
Drop in blood pressure and fluid induce this mechanism.
THE JUXTAGLOMERULAR APPARATUS
The renin in kidney extracts and the bloodstream is produced by the
juxtaglomerular cells (JG cells)
Renin converts angiotensinogen (produced by the liver) into angioten
then converted to angiotensin II (a potent vasoconstrictor) by the ang
converting enzyme (ACE). Angiotensin II stimulates aldosterone relea
adrenal glands, promoting sodium and water retention. Homeostasis:
blood pressure stability and proper blood volume.
z
Clinical cor
1.Hypertension
High Renin Hypertension: Conditions with elevated renin levels often lead to secondary hype
Renovascular hypertension (e.g., renal artery stenosis)
Malignant hypertension
Certain forms of essential hypertension
Low Renin Hypertension: Often associated with:
Primary hyperaldosteronism (e.g., Conn's syndrome)
Liddle syndrome
Cushing’s syndrome
Chronic kidney disease
Clinical Use: Measuring renin and aldosterone levels helps distinguish between primary and
of hypertension
13.
z
Renal arterystenosis lead to reduced renal perfusion
stimulating renin release. This results in secondary
hyperaldosteronism, causing hypertension and hypok
Renin levels are often elevated.
In heart failure, reduced cardiac output leads to decre
perfusion, stimulating renin release. This can exacerb
retention and worsen symptoms.
Renin inhibitors (e.g., aliskiren) or RAAS blockers (AC
inhibitors, ARBs) are used therapeutically.
14.
z
C
Laboratory Assessment
Plasma ReninActivity (PRA): Reflects the enzymatic act
renin converting angiotensinogen to angiotensin I.
Direct Renin Concentration (DRC): Measures the amoun
in the blood.
Testing often includes aldosterone measurements to cal
aldosterone-to-renin ratio (ARR).
15.
z
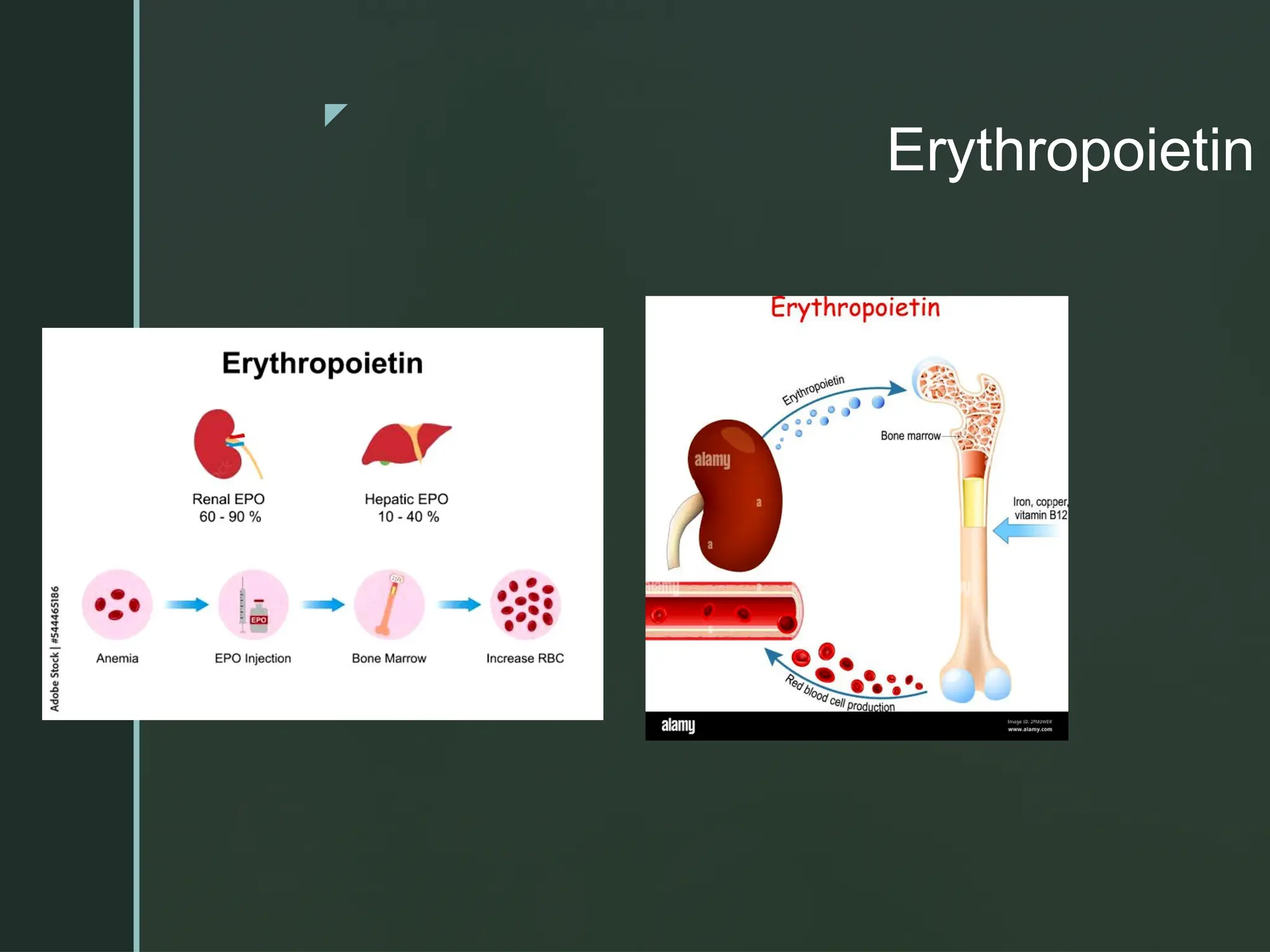
Erythropoietin
Role: Stimulatesred blood cell production in the bone marrow in response to
levels (hypoxia).
Erythropoitin is a peptide hormone which regulates Erythropoiesis
Homeostasis: Helps maintain adequate oxygen delivery to tissues by regula
cell levels.
In adults, about 85% of the erythropoietin comes from the kidneys and 15%
Both these organs contain the mRNA for erythropoietin.
Erythropoietin can also be extracted from the spleen and salivary glands, bu
do not contain its mRNA and consequently do not appear to manufacture the
Erythropoietin is produced by interstitial cells in the peritubular capillary bed
and by perivenous hepatocytes in the liver.
z
Erythropoietin
Clinical correlations
For most people in end stage renal failure,anaemia w
erythropoietin deficiency occurs.
Can administer Recombinant erythropoietin to these
19.
z
Anemia
Anemiaof Chronic Disease or Preoperative Anemia: Ma
patients present with anemia, which increases the risk o
perioperative complications. Administering recombinant
erythropoietin (rHuEPO) preoperatively, often alongside
supplementation, can boost hemoglobin levels and redu
need for blood transfusions during surgery.
Orthopedic or Cardiac Surgery: EPO is particularly bene
major surgeries, such as joint replacements or cardiac p
where blood loss is anticipated.
20.
z
Reduction inAllogeneic Blood Transfusions
Allogeneic blood transfusions are associated with risks such as infections,
reactions, and fluid overload.
Using EPO reduces the dependency on transfusions by enhancing the pa
erythropoietic response.
Chronic Kidney Disease (CKD): CKD patients often have low baseline EPO
to anemia. Recombinant EPO is critical for managing their anemia before a
surgery.
Cancer Surgery: EPO may be used cautiously in cancer patients undergoin
anemia is common in this population, though concerns about tumor progre
thrombosis exist
21.
z
Risks andLimitations
Thromboembolic Events: EPO increases the risk of v
thromboembolism, especially in patients with high he
targets.
Hypertension: EPO can exacerbate hypertension, wh
requires careful monitoring perioperatively.
Optimal Timing: The administration of EPO typically r
weeks to elevate hemoglobin levels effectively, so it m
suitable for urgent surgeries
22.
z
Calcitriol (Active Vitam
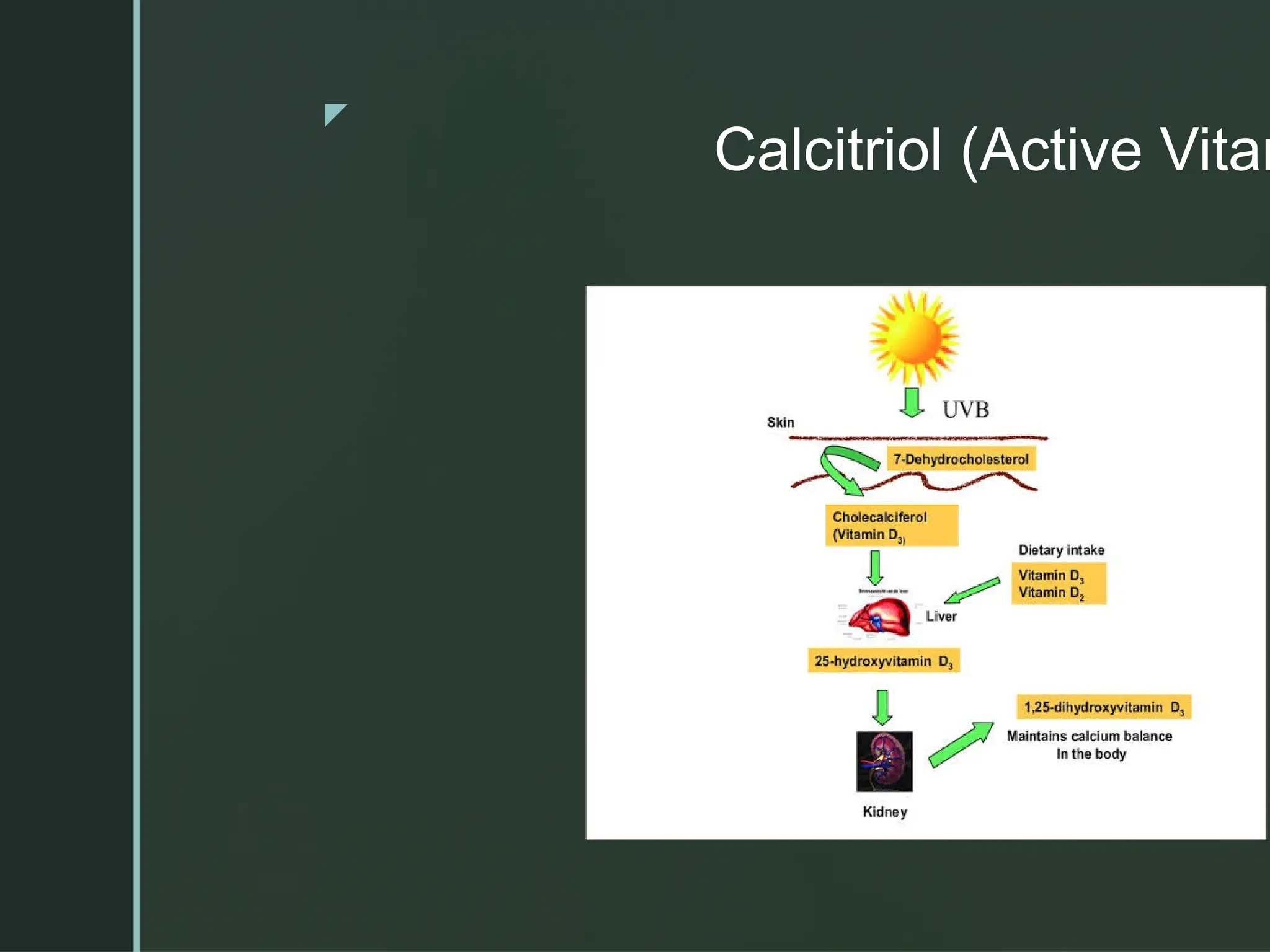
Calcitriol (Active Vitamin D): Role: Promotes calcium and
phosphate absorption in the intestines, regulates bone
mineralization, and modulates parathyroid hormone (PTH)
levels.
Homeostasis: Maintains calcium and phosphate balance,
crucial for bone health and neuromuscular function
z
CLNICAL CORREL
Afterparathyroidectomy; hypocalcemia (hungry bone syndrome) may devel
rapidly uptake calcium. Calcitriol is often administered postoperatively to en
calcium absorption and mitigate hypocalcemia.
Renal Transplantation
Post-Transplant Hypocalcemia:
Patients with chronic kidney disease (CKD) often have suppressed calcitriol
reduced renal conversion of 25-hydroxyvitamin D to calcitriol.
Post-surgery, calcitriol supplementation is crucial for restoring calcium-phos
Bone Health:
Calcitriol is used to manage secondary hyperparathyroidism and prevent ren
osteodystrophy.
25.
z
Bone Healing:
Calcitriol promotes bone healing by enhancing calciu
phosphate deposition in bone matrix. In patients with
deficiency or osteoporosis, calcitriol supplementation
improve surgical outcomes.
Fracture Repair:
Adequate calcitriol levels are essential for proper min
and repair of fractures
26.
z
Monitoring: Regularmonitoring of calcium, phosphoru
PTH levels is critical when using calcitriol in periopera
settings.
Dose Adjustment: Overuse of calcitriol can lead to
hypercalcemia and hyperphosphatemia, potentially ca
nephrocalcinosis or vascular calcifications.
Vitamin D Deficiency: Surgeons should assess and c
vitamin D deficiency preoperatively to optimize surgic
outcomes.
27.
z
SUM
Recap:
Kidneysare essential for homeostasis.
Renal hormones regulate Blood pressure
red blood cell production.
Mineral balance.
Dysregulation can lead to serious health issues.
Hypertension
Anemia
Vitamin D deficiency.