Downloaded 12 times

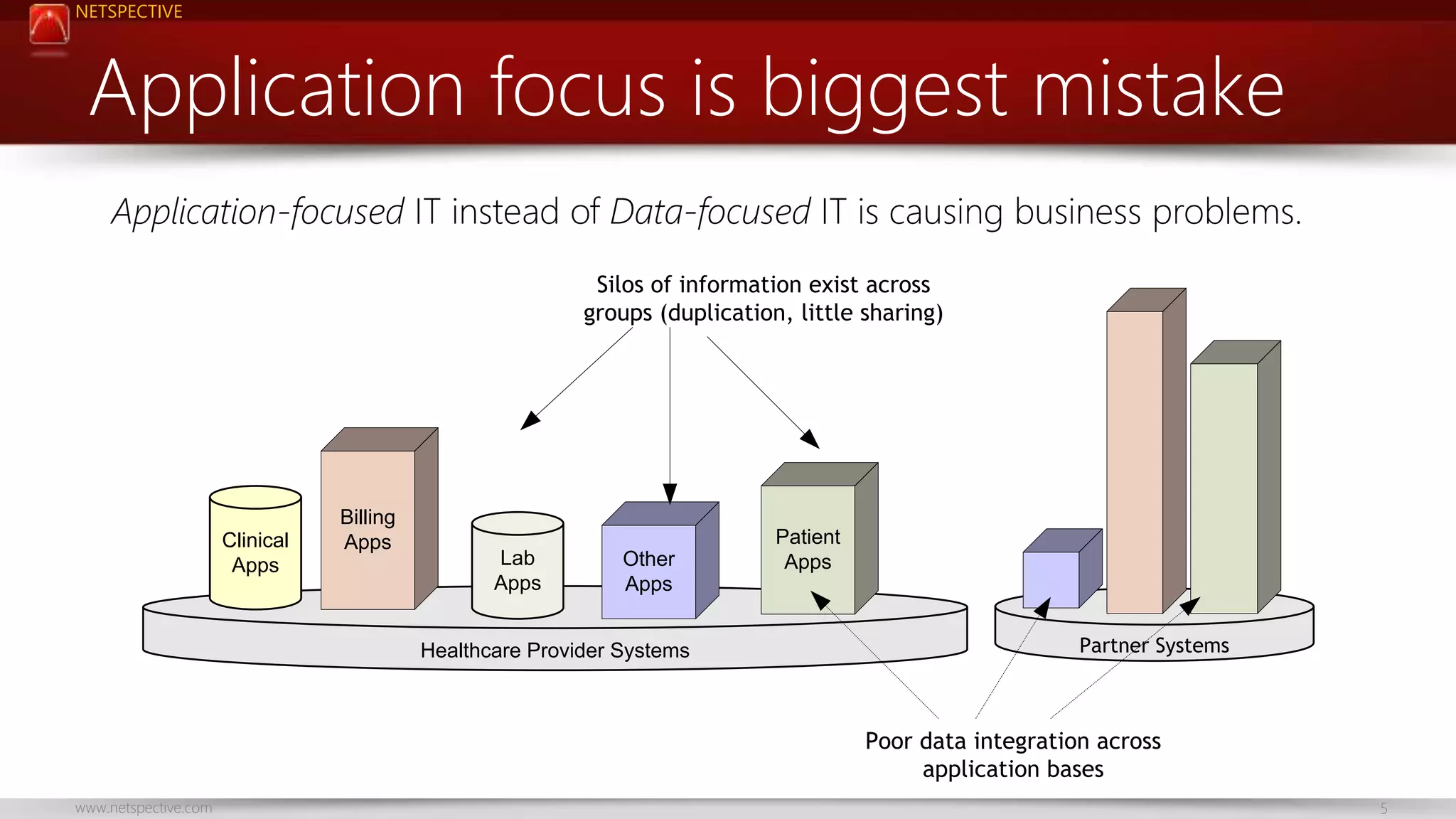
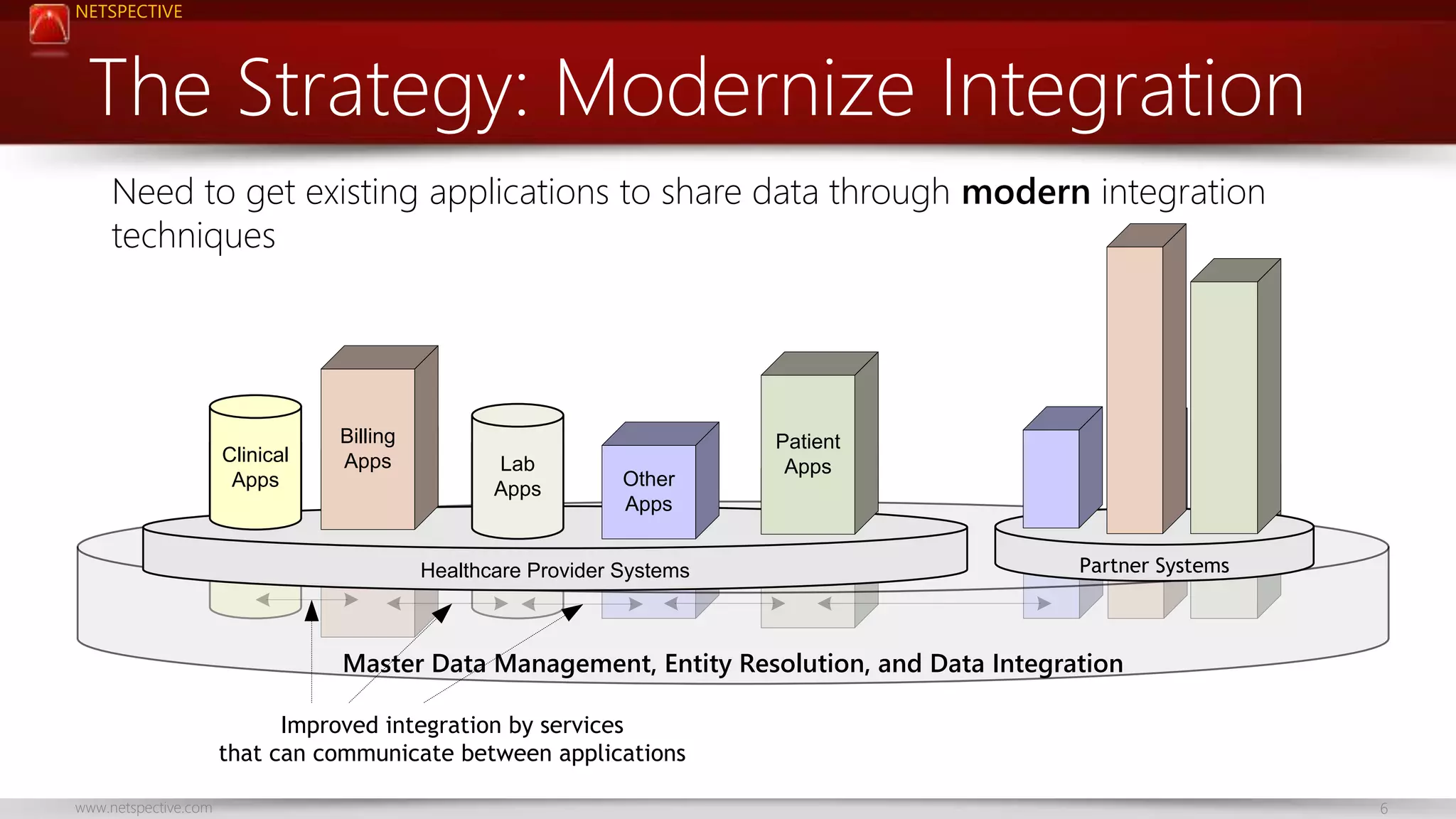
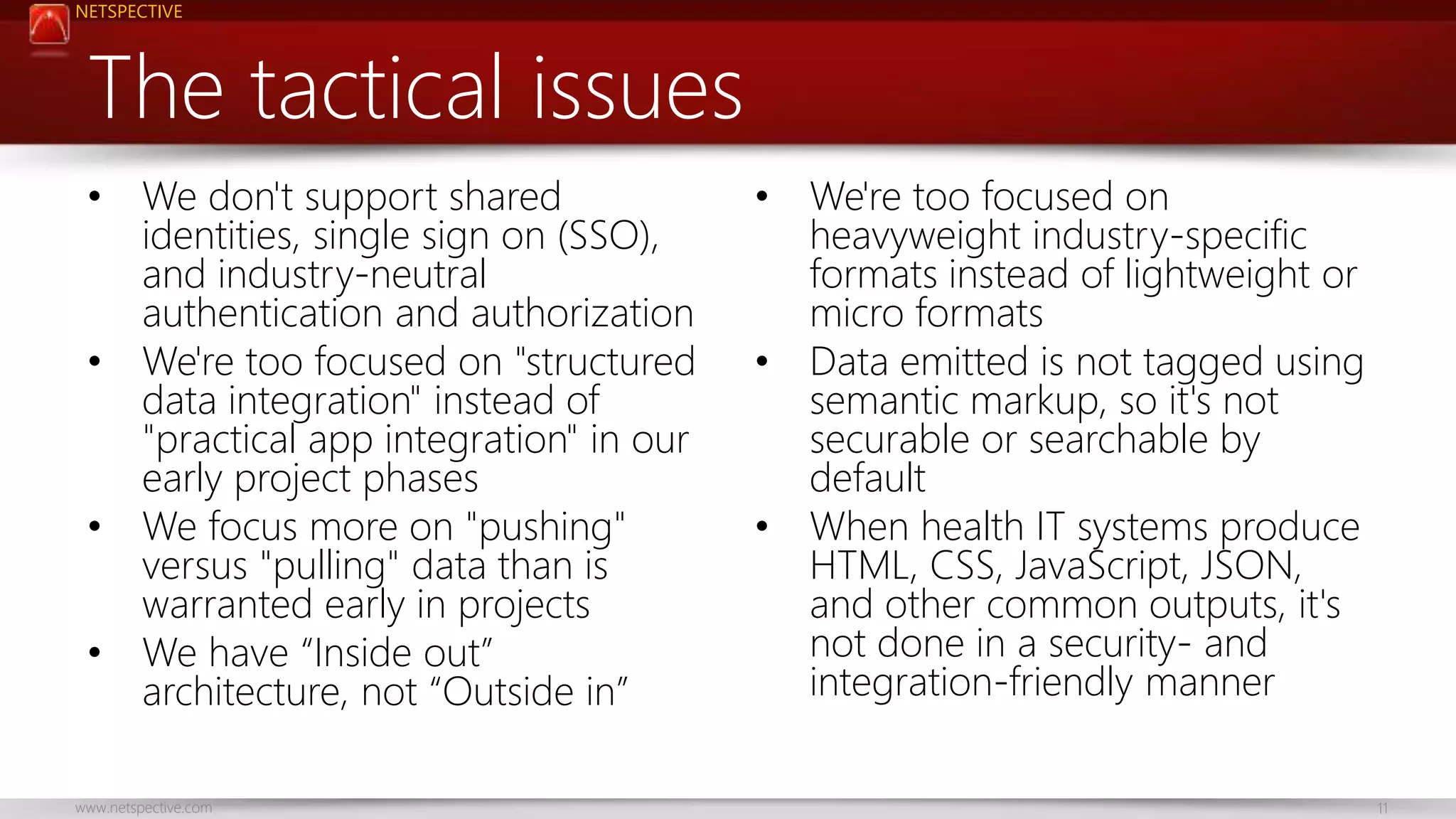


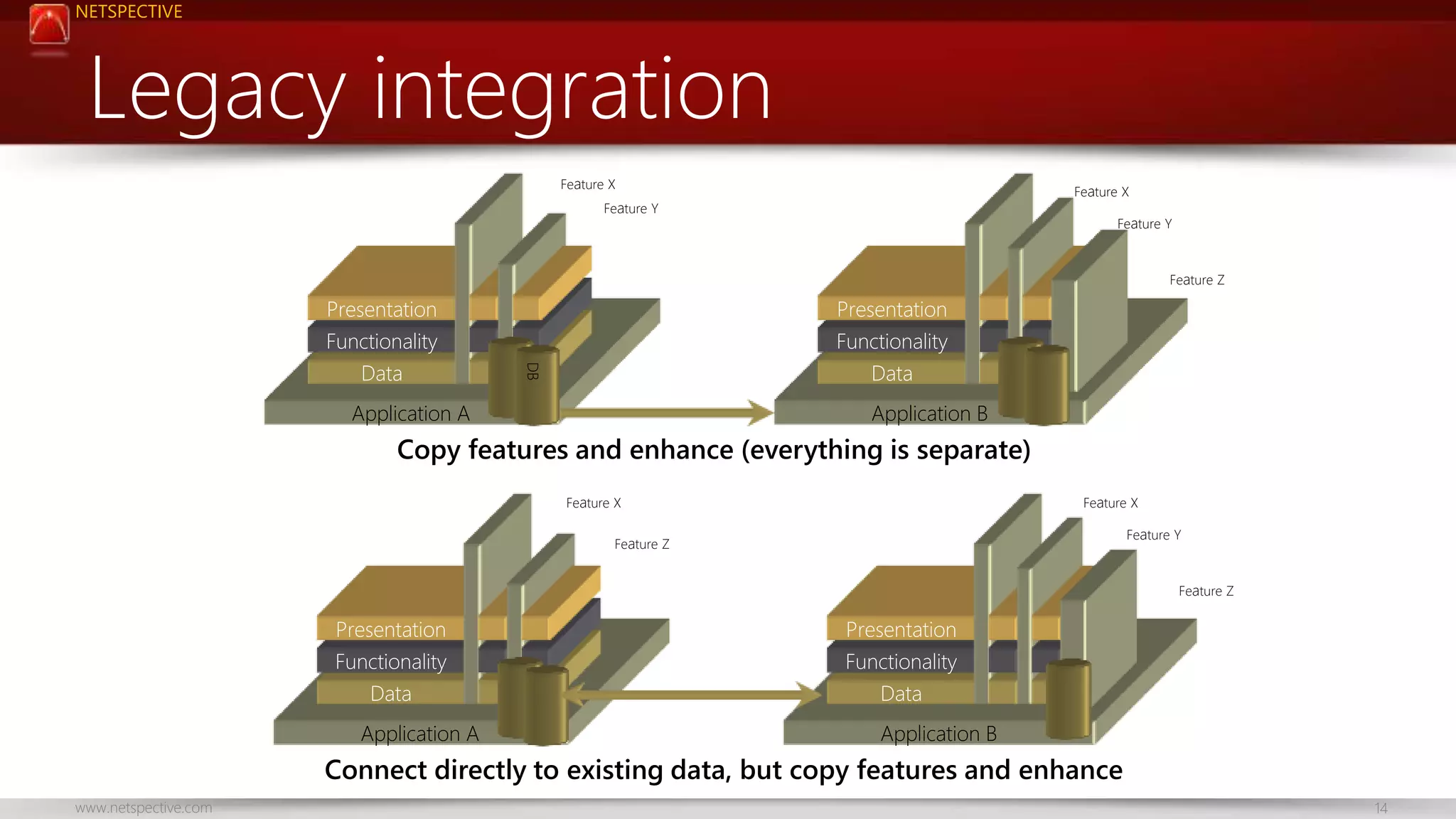
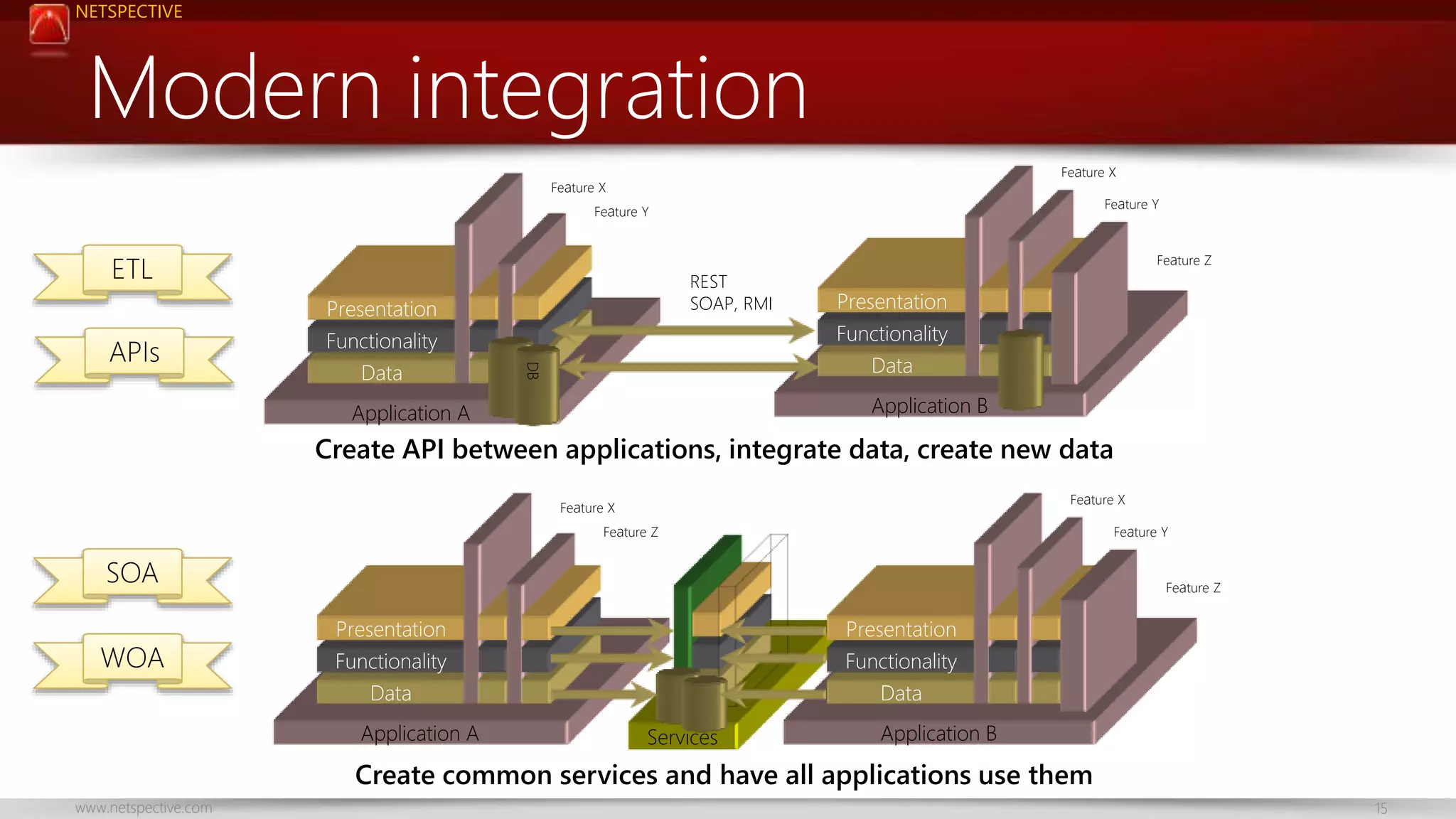

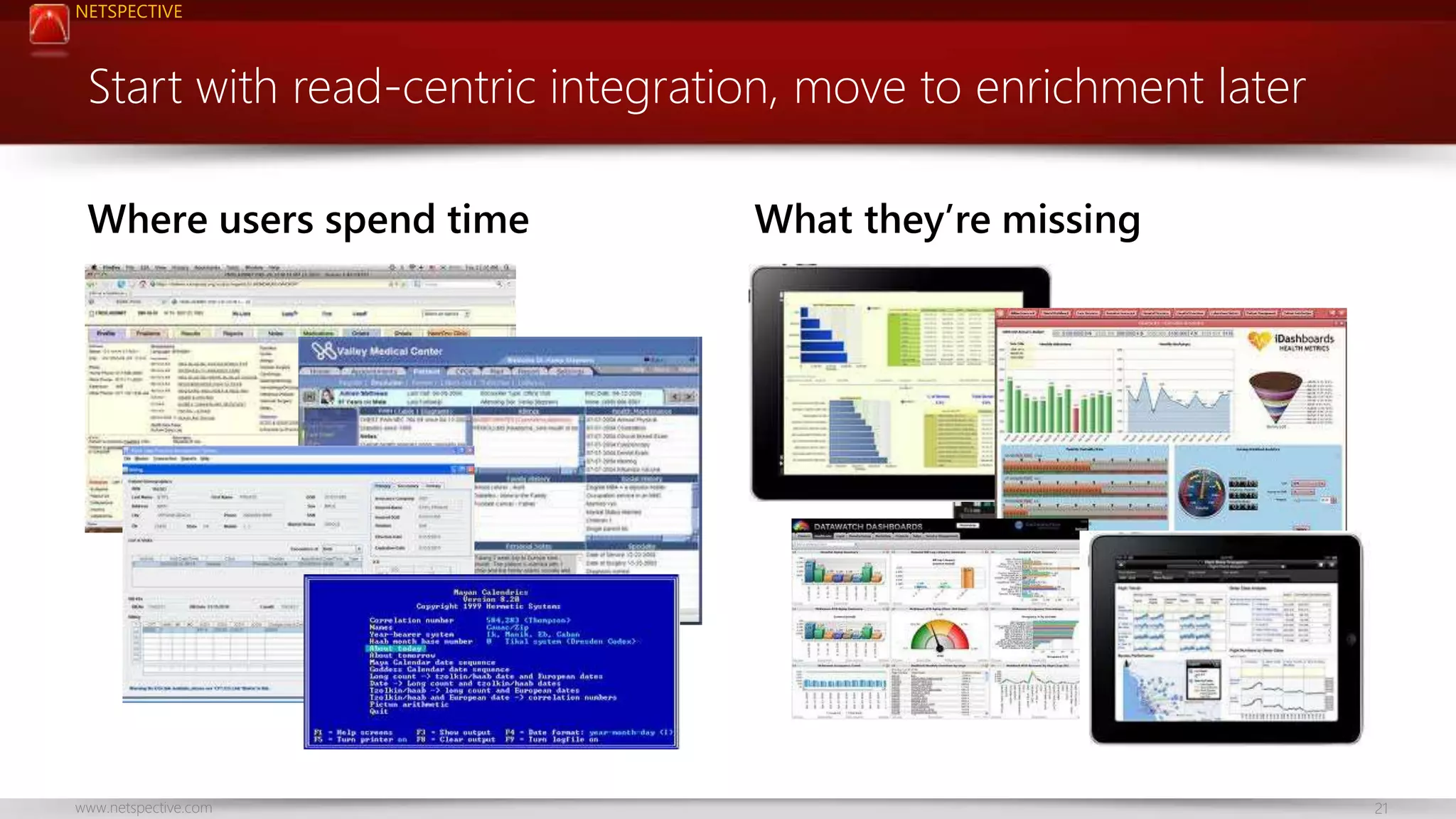
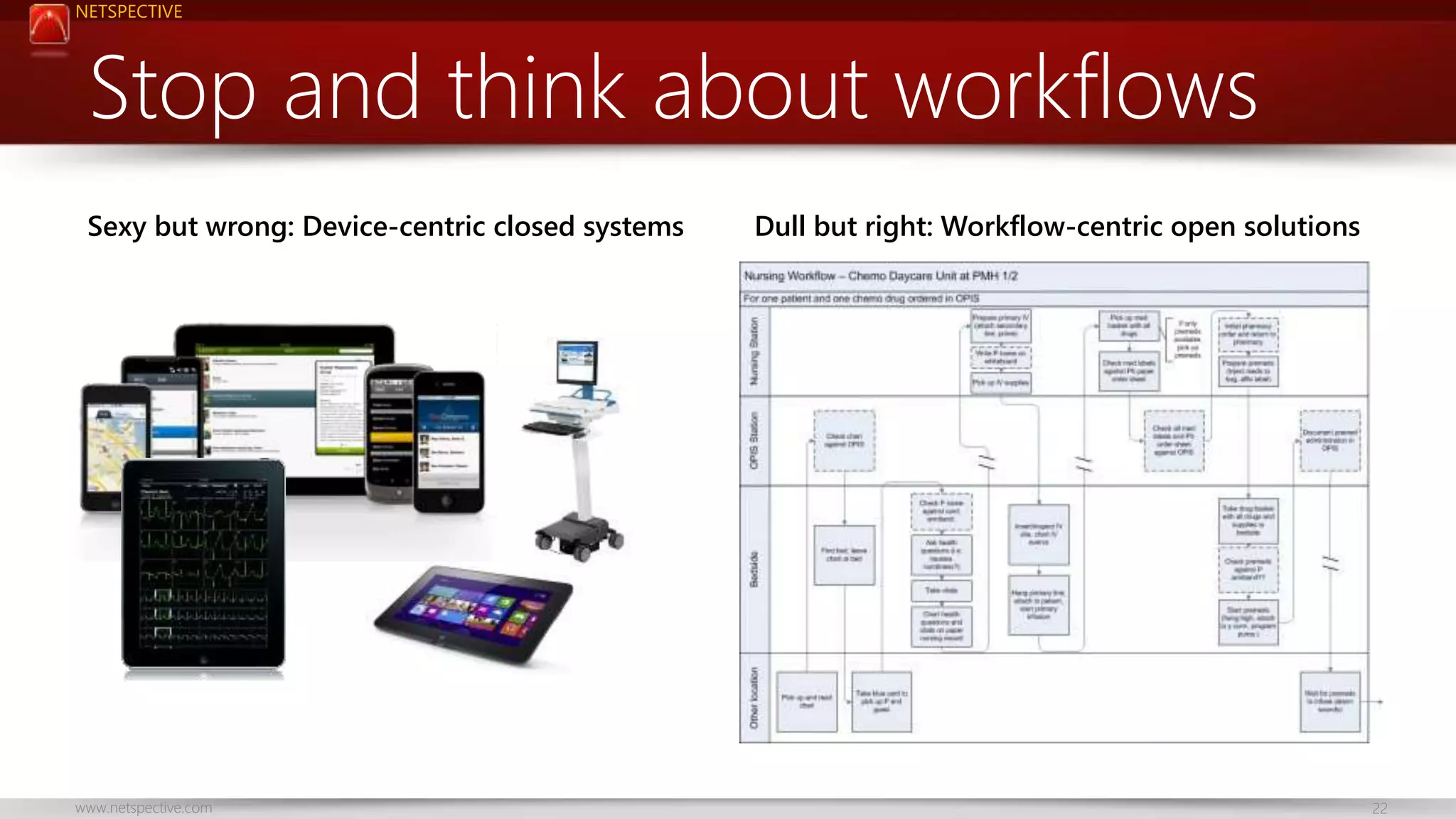
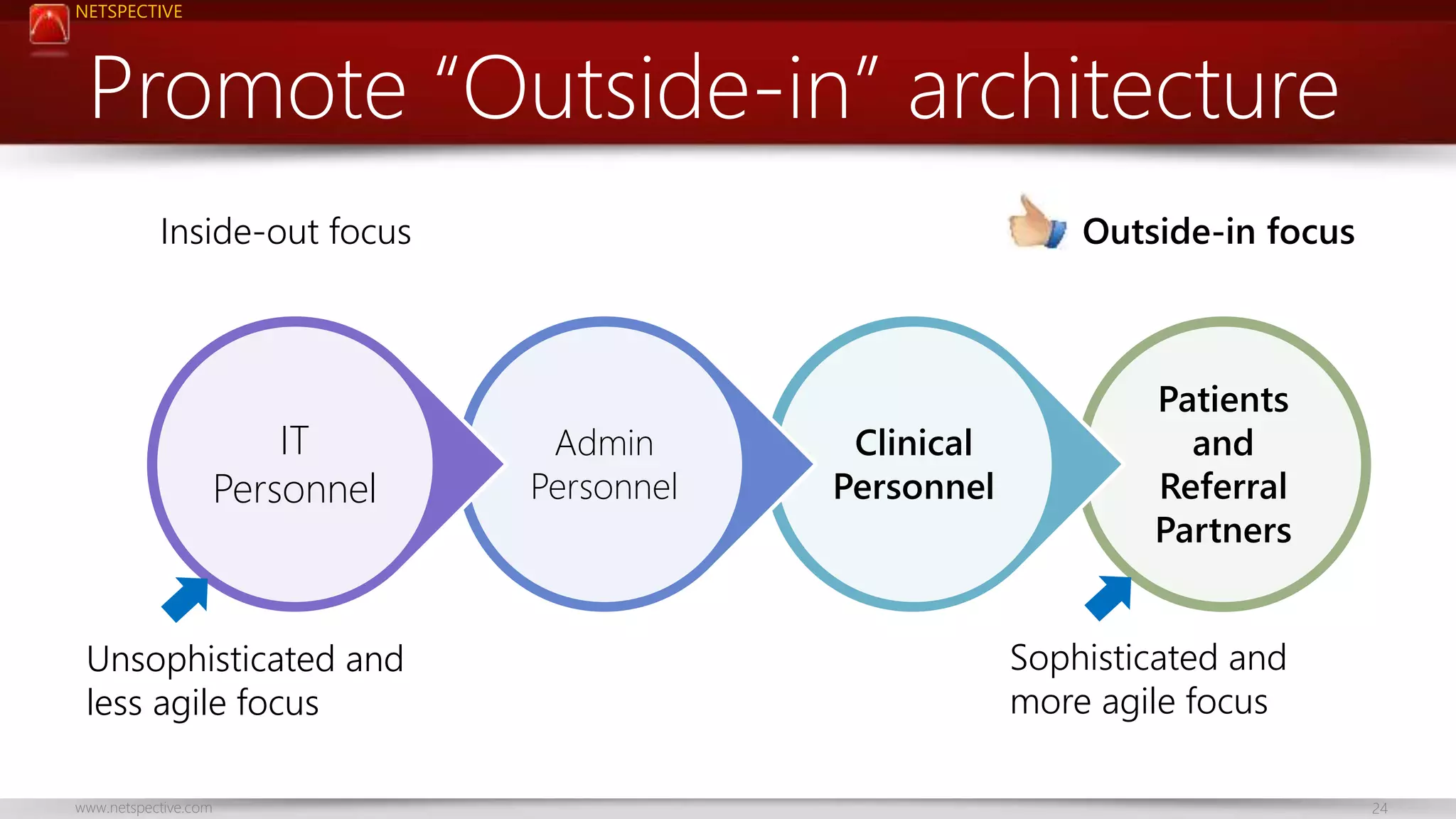


The document discusses the challenges of integrating health data effectively, highlighting that many healthcare applications function as standalone systems and fail to share data properly. It emphasizes the need for a shift towards data-focused integration strategies and the adoption of industry-neutral technologies to improve interoperability. The presentation outlines tactical issues, potential solutions, and best practices for enhancing data integration within healthcare IT systems.










































































