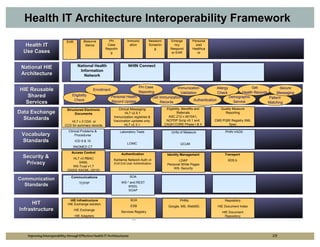
The document outlines strategies for improving interoperability in health IT architecture, addressing current challenges and the importance of effective communication between health systems. It emphasizes the necessity of adopting national standards, reusable shared services, and governance to enhance data exchange. The document also discusses various levels of interoperability and the role of public health IT systems in achieving these goals.