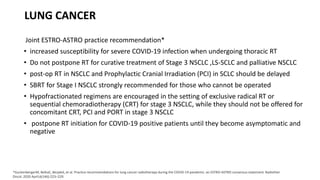
This document discusses considerations for delivering radiotherapy to cancer patients during the COVID-19 pandemic. It outlines how cancer patients are at high risk for severe COVID-19 outcomes. Recommendations are made to prioritize the most urgent cases based on tumor type and stage. Practical strategies are suggested to minimize risks, including hypofractionation where possible, delaying elective treatments, and stringent infection control measures. Guidance is provided specifically for lung, rectal, prostate cancers and other sites based on balancing COVID-19 risks with cancer treatment needs.


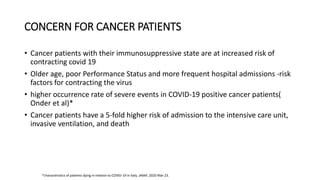
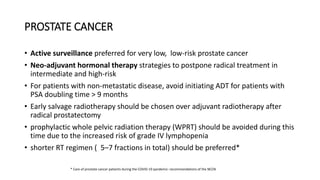
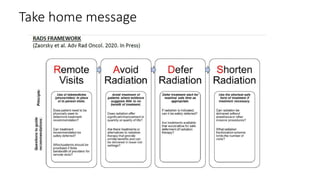
![• Defer initial post-treatment monitoring (PSA-based testing and digital rectal exam
[DRE]) until deemed safe
• Consideration to use 3-, 4-, or 6-month formulations of ADT should be preferred
over 1-month injections
• Defer repeat imaging over time if PSA is declining and absence of symptoms until
risk of COVID-19 has resolved.](https://image.slidesharecdn.com/radiotherapyincovidera-200827102203/85/Radiotherapy-in-covid-era-19-320.jpg)





















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






