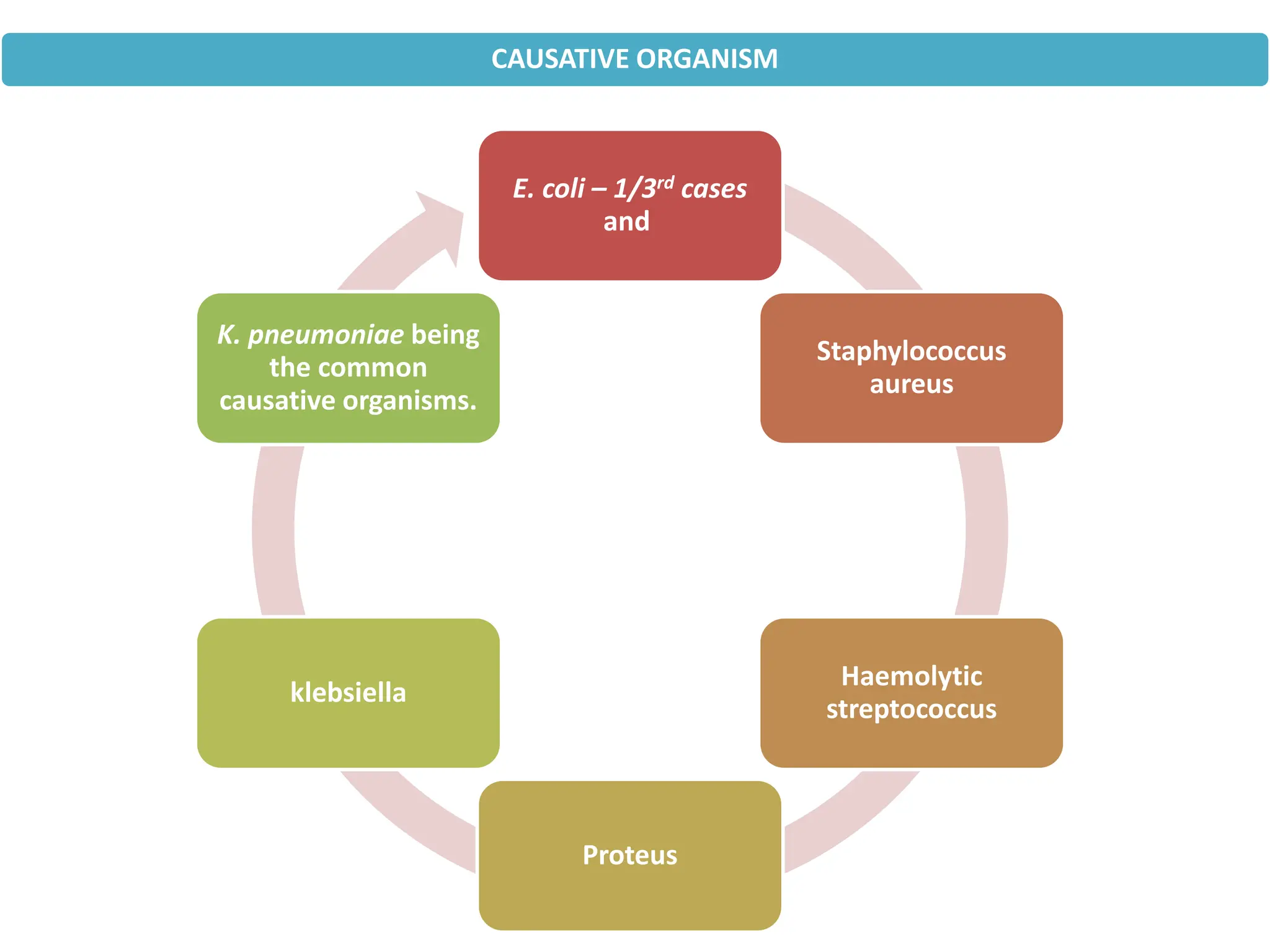
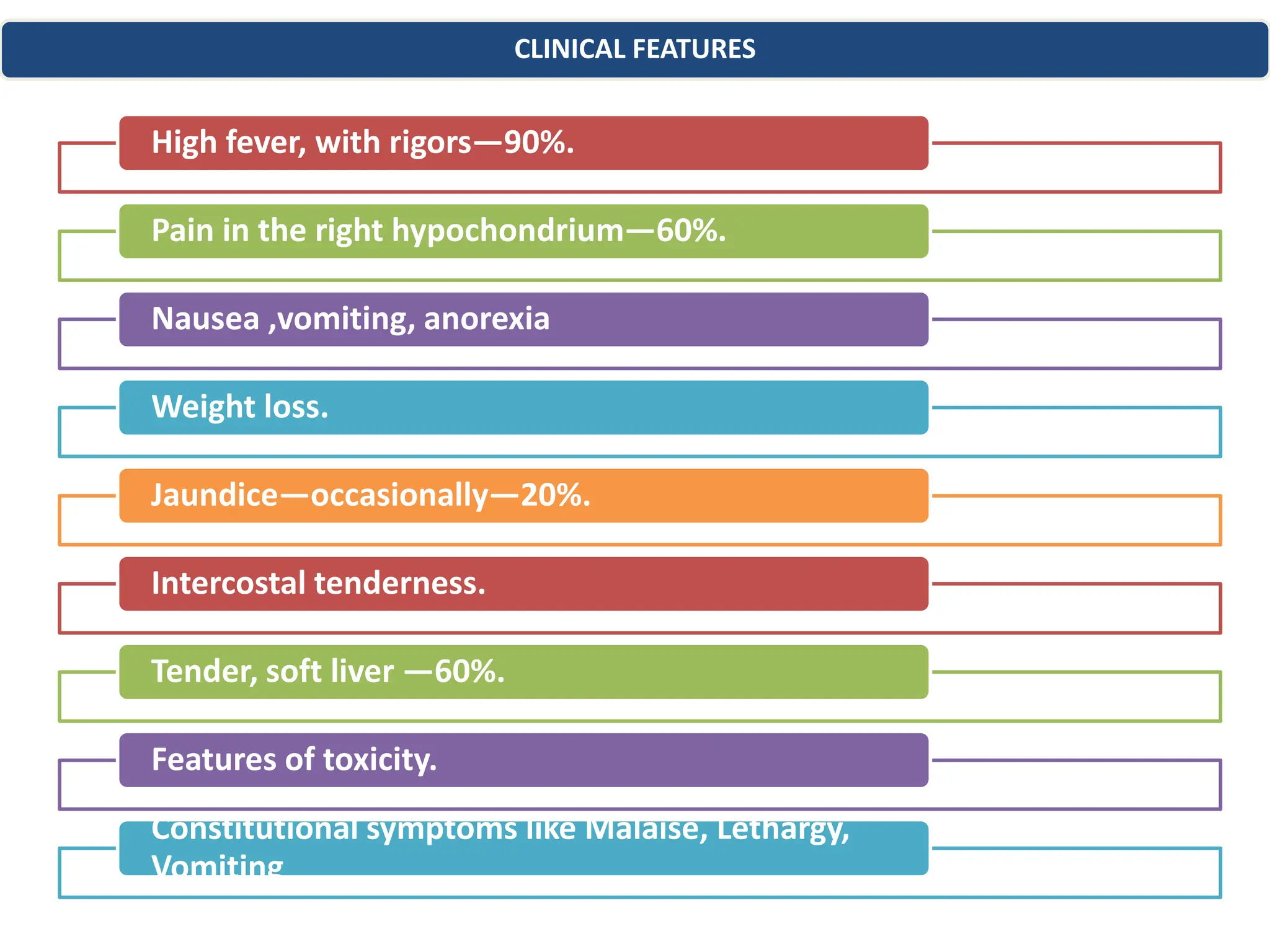
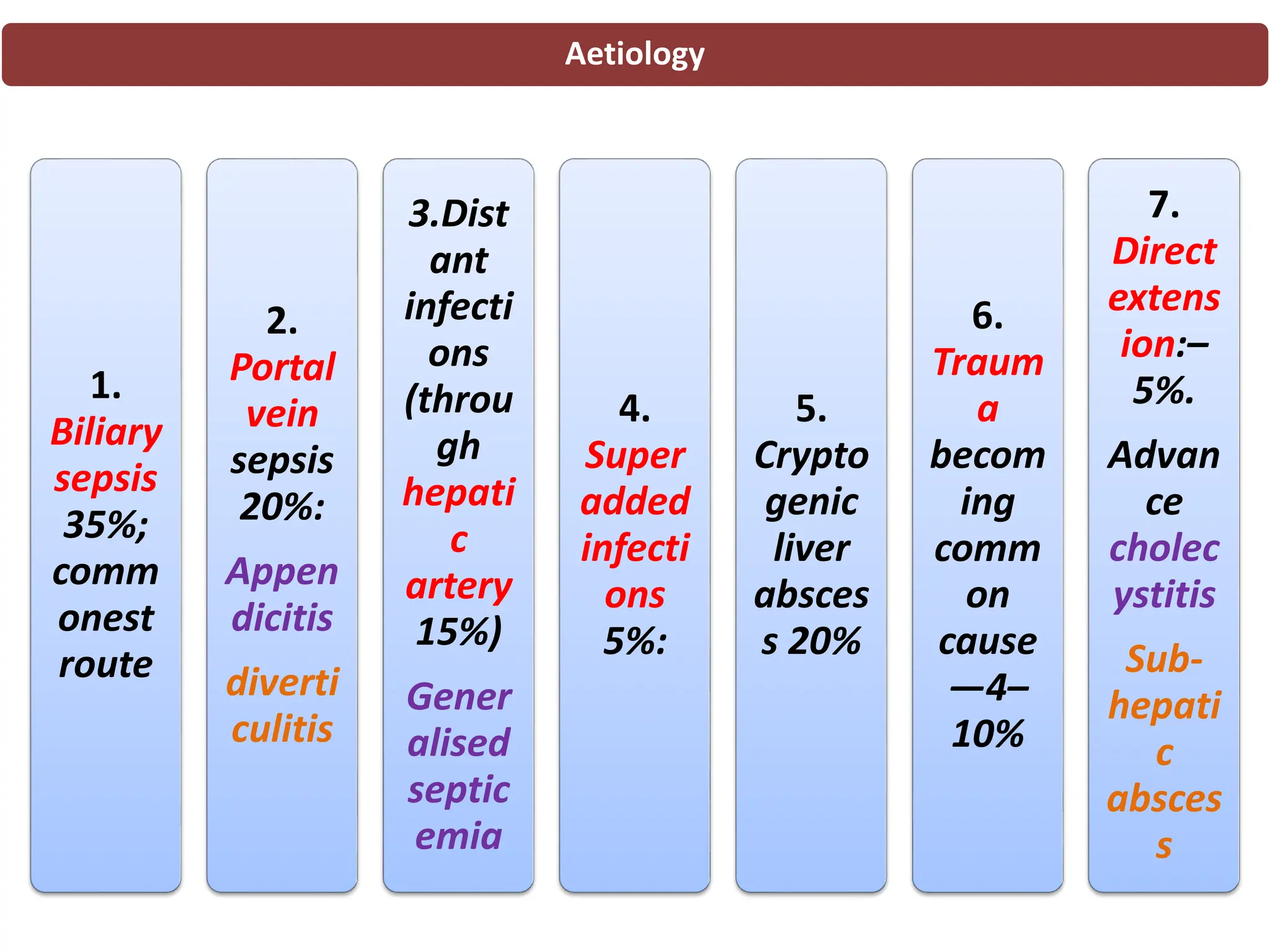
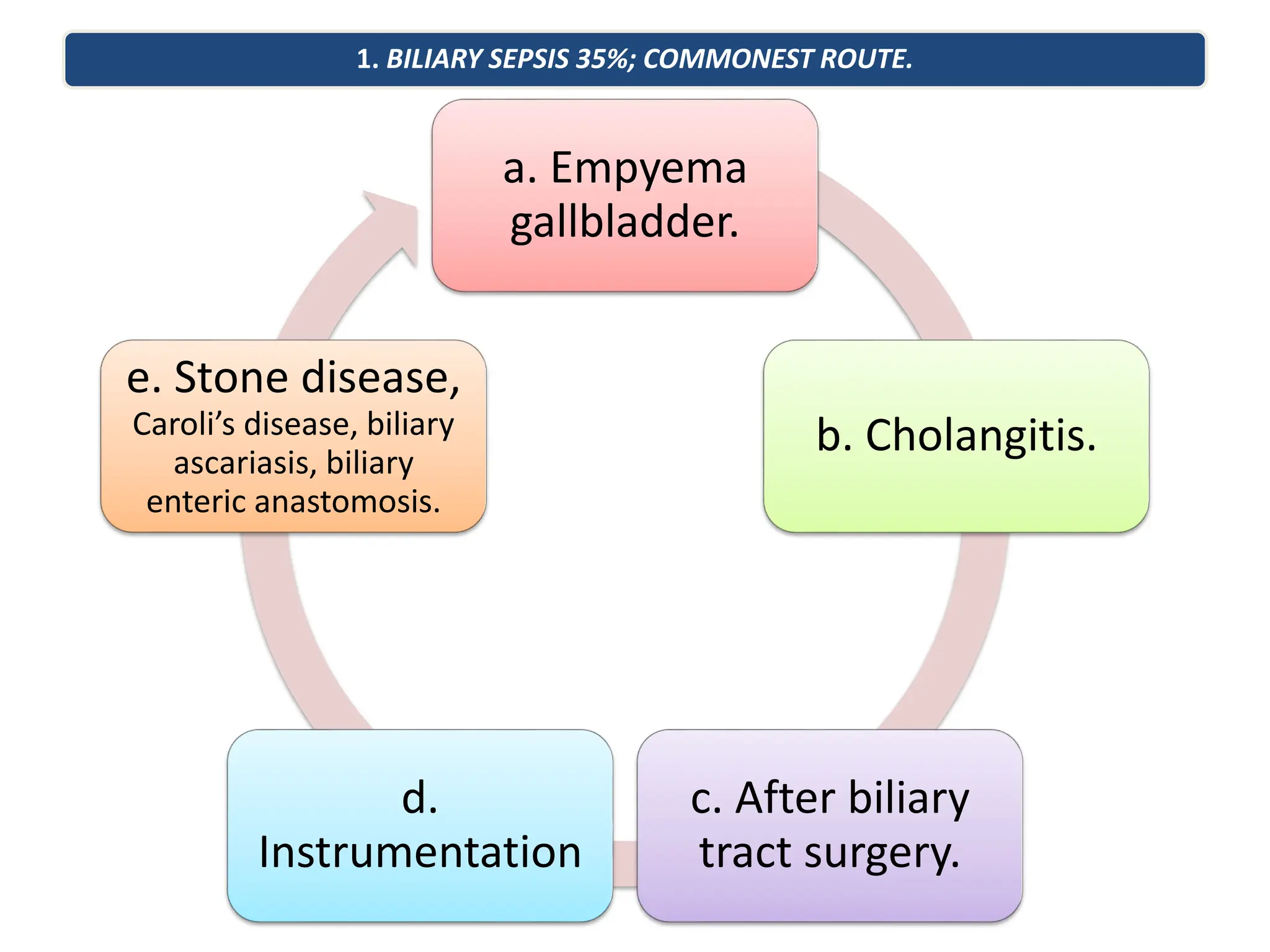
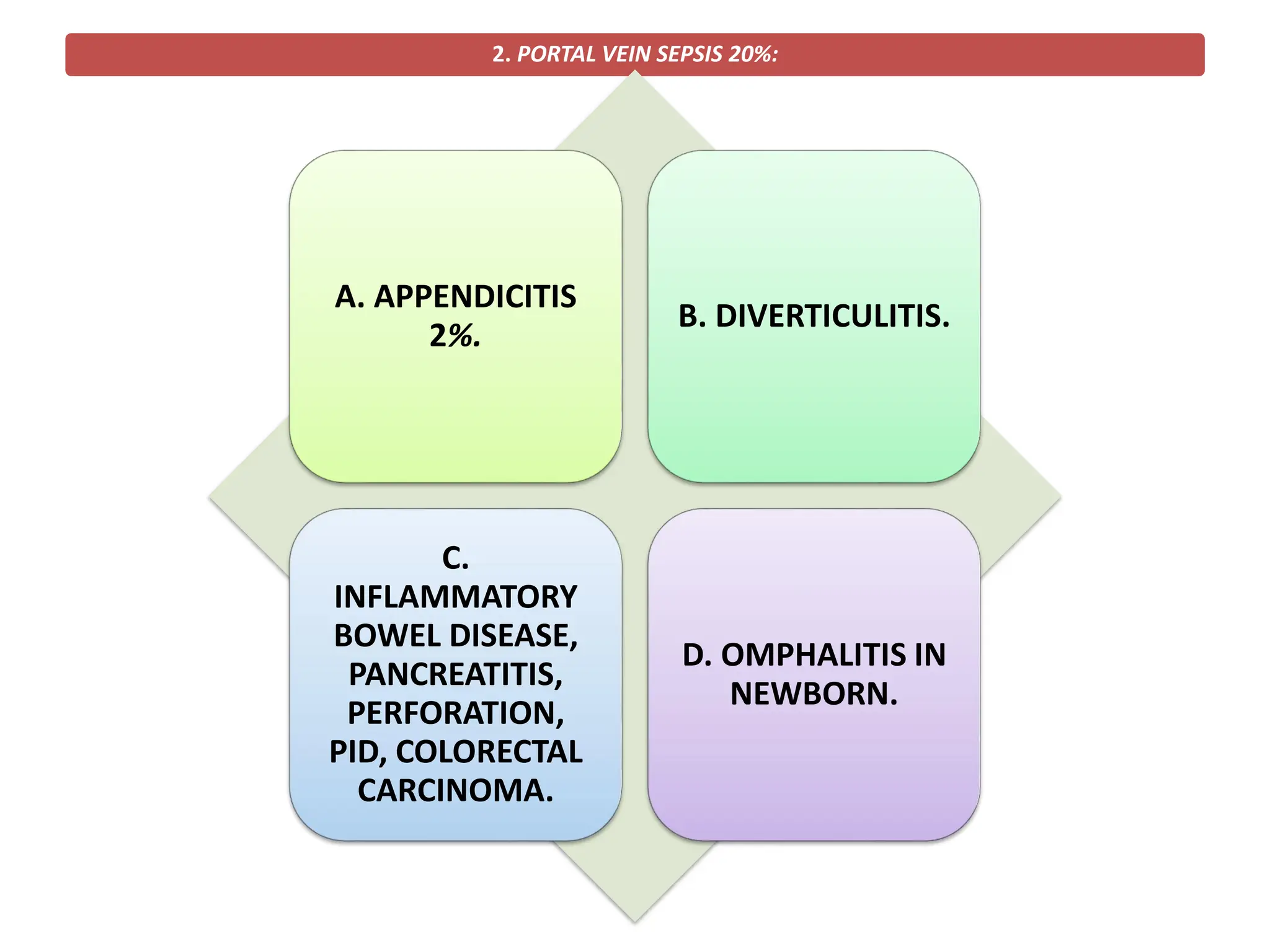
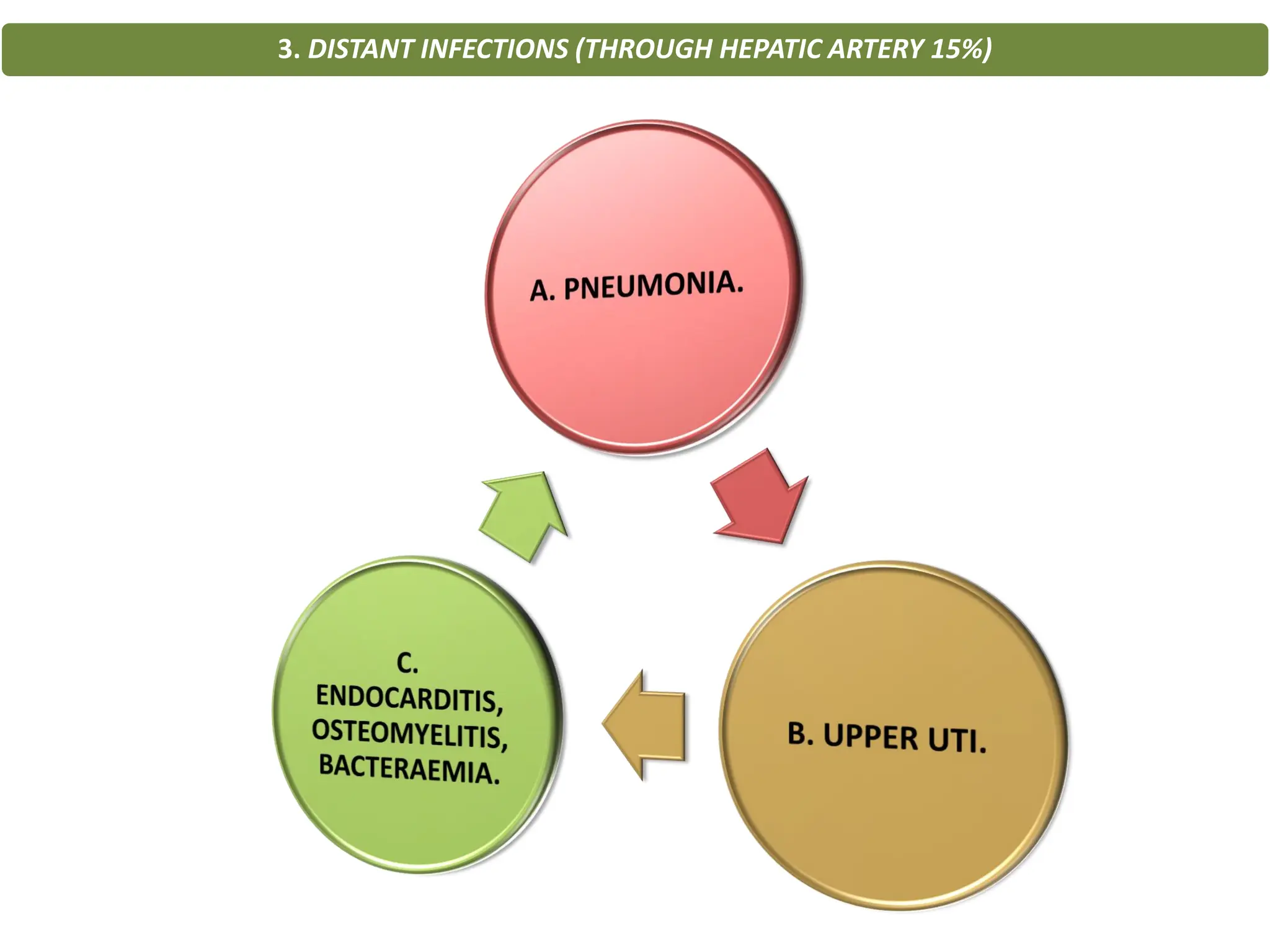
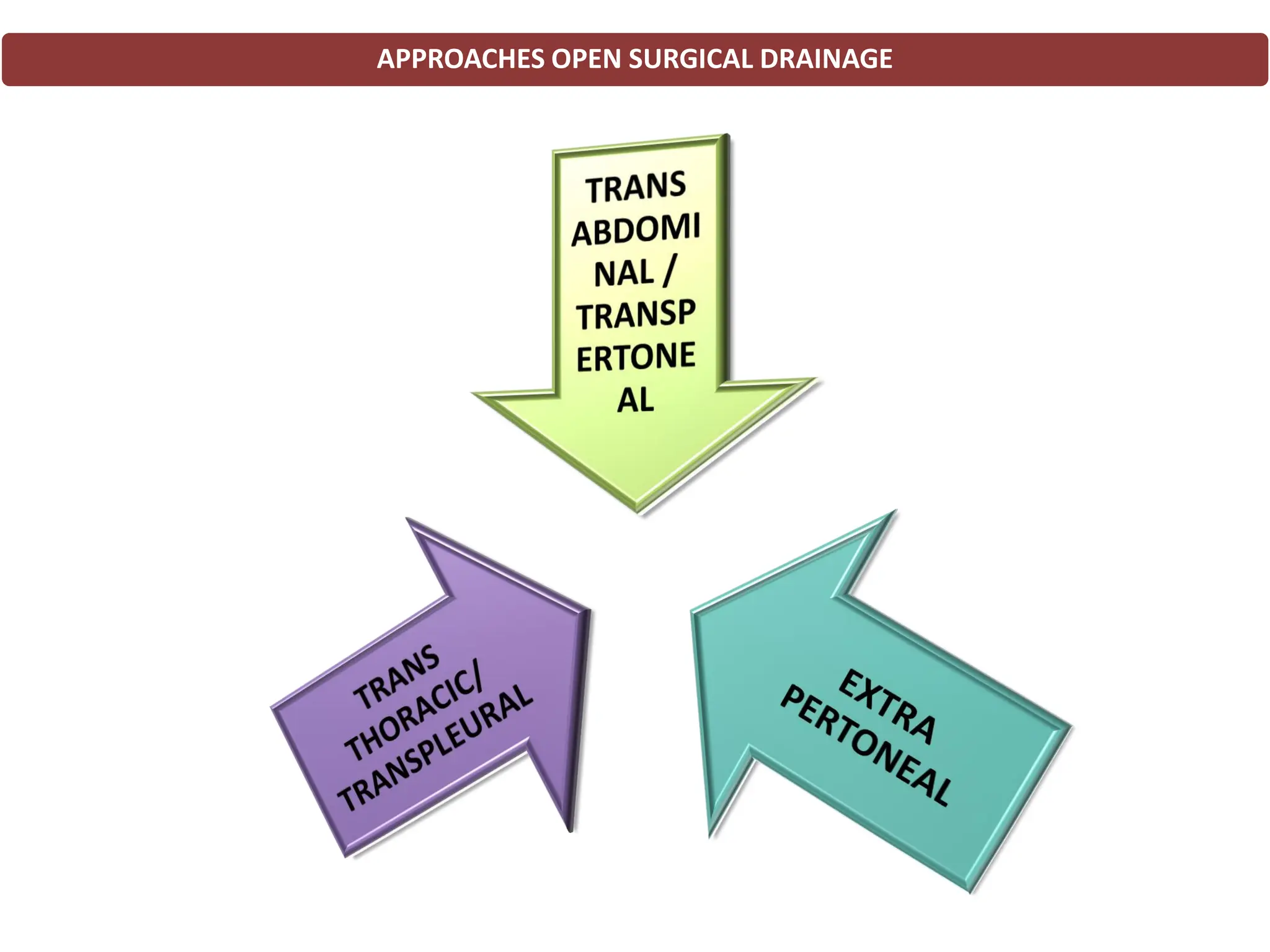
A pyogenic liver abscess is a rare condition characterized by pus collections in the liver, commonly caused by bacteria such as E. coli and Staphylococcus aureus. Symptoms include high fever, abdominal pain, and general malaise, with differential diagnoses and treatment options involving antibiotics and drainage methods. The condition's prognosis is poor without drainage, leading to potential complications such as septicemia and liver failure.