Downloaded 186 times


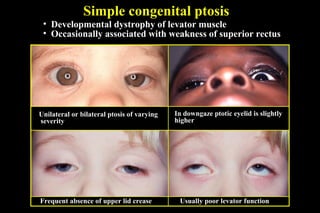
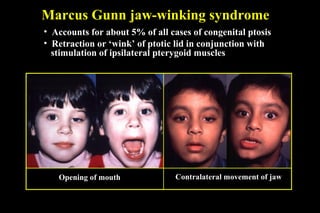
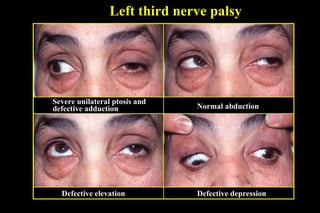
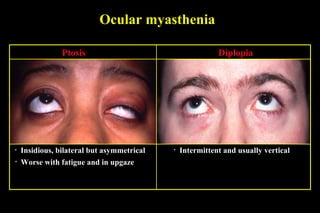
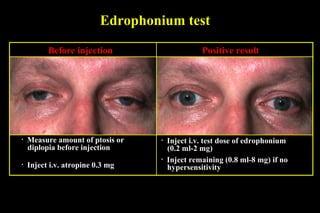
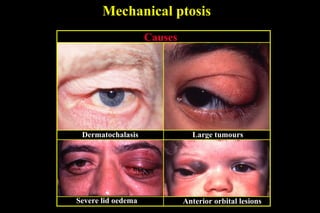
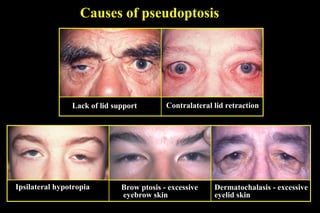

1) Ptosis is an abnormally low position of the upper eyelid that can be congenital or acquired. Congenital ptosis is usually bilateral and hereditary, caused by defective development of the levator palpebrae superioris muscle. Acquired ptosis has several causes including neurogenic (e.g. third nerve palsy), myogenic (e.g. myasthenia gravis), aponeurotic, or mechanical factors like tumors. 2) Myasthenia gravis is tested for using edrophonium, which temporarily improves ptosis and diplopia. Marcus Gunn jaw-winking syndrome is a rare form of congenital ptosis where the eyel








































![CLINICAL EVALUATION AND MANAGEMENT OPTION OF AQUIRED PTOSIS [Autosaved]_09133...](https://cdn.slidesharecdn.com/ss_thumbnails/clinicalevaluationandmanagementoptionofaquiredptosisautosaved091336-250701164538-7d28272b-thumbnail.jpg?width=640&height=640&fit=bounds)


























