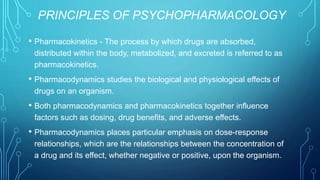
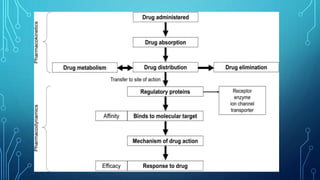
Psychopharmacology studies the effects of drugs on the nervous system and behavior, covering areas such as pharmacokinetics, pharmacodynamics, and drug administration routes. Drug effectiveness is influenced by factors like dosage, affinity for receptor sites, and potential for tolerance and sensitization, while various drug delivery methods impact the speed and efficiency of drug action. Additionally, the interaction between drugs and neurotransmitters can either inhibit or facilitate synaptic transmission, resulting in complex behavioral outcomes.