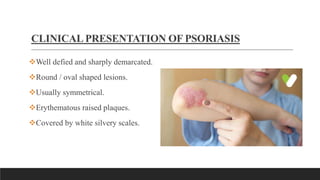
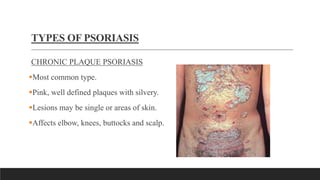
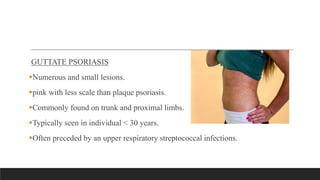
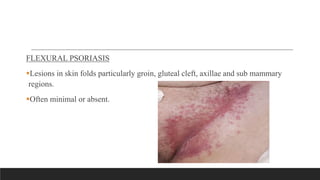
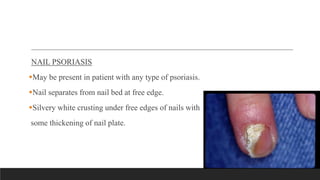
Psoriasis presents with well-defined, raised, erythematous plaques covered with silvery scales that are usually symmetrical. The most common type is chronic plaque psoriasis, characterized by pink plaques on the elbows, knees, scalp and back. Guttate psoriasis causes many small lesions, often after a streptococcal infection, while flexural psoriasis affects skin folds. Treatment includes topical emollients, keratolytics like coal tar to remove scales, and corticosteroids to reduce inflammation. Nursing diagnoses include impaired skin integrity from lesions and itching, risk of infection from loss of fluid and protein, and acute pain from inflammation.