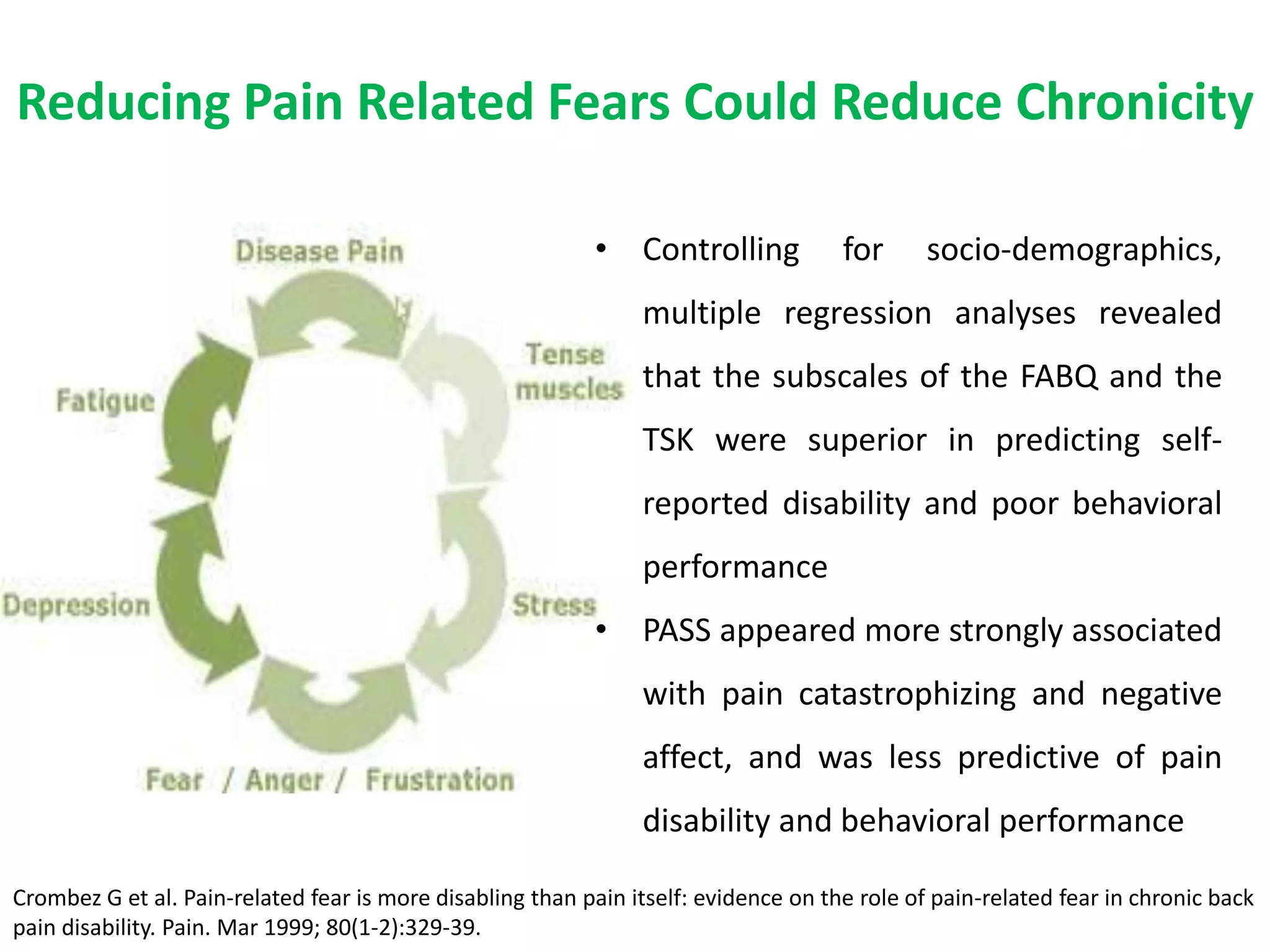
1. Preventing acute pain from transitioning to chronic pain requires early intervention, as chronic pain is defined as persisting over 3 months and is associated with physiological and psychological changes.
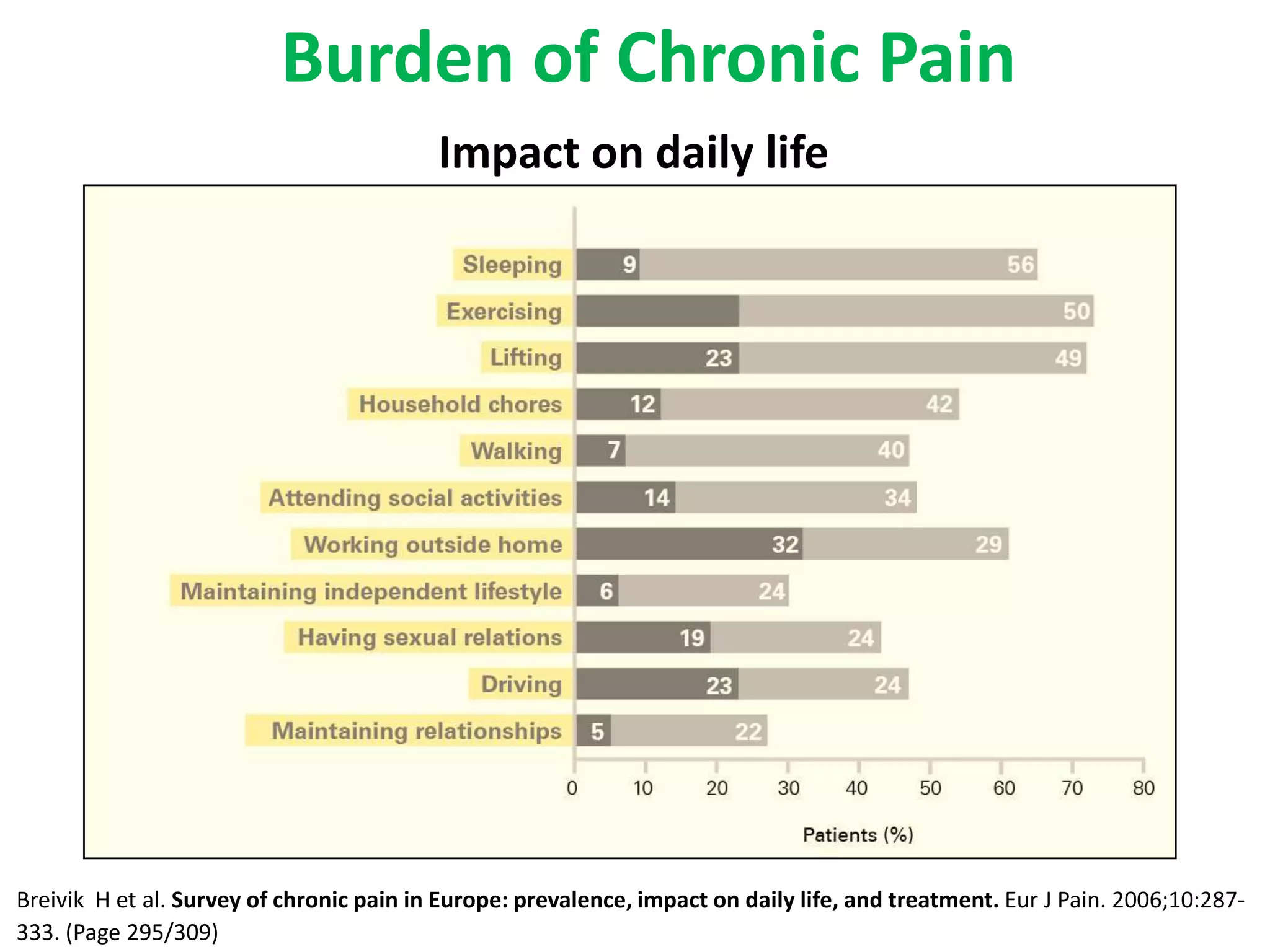
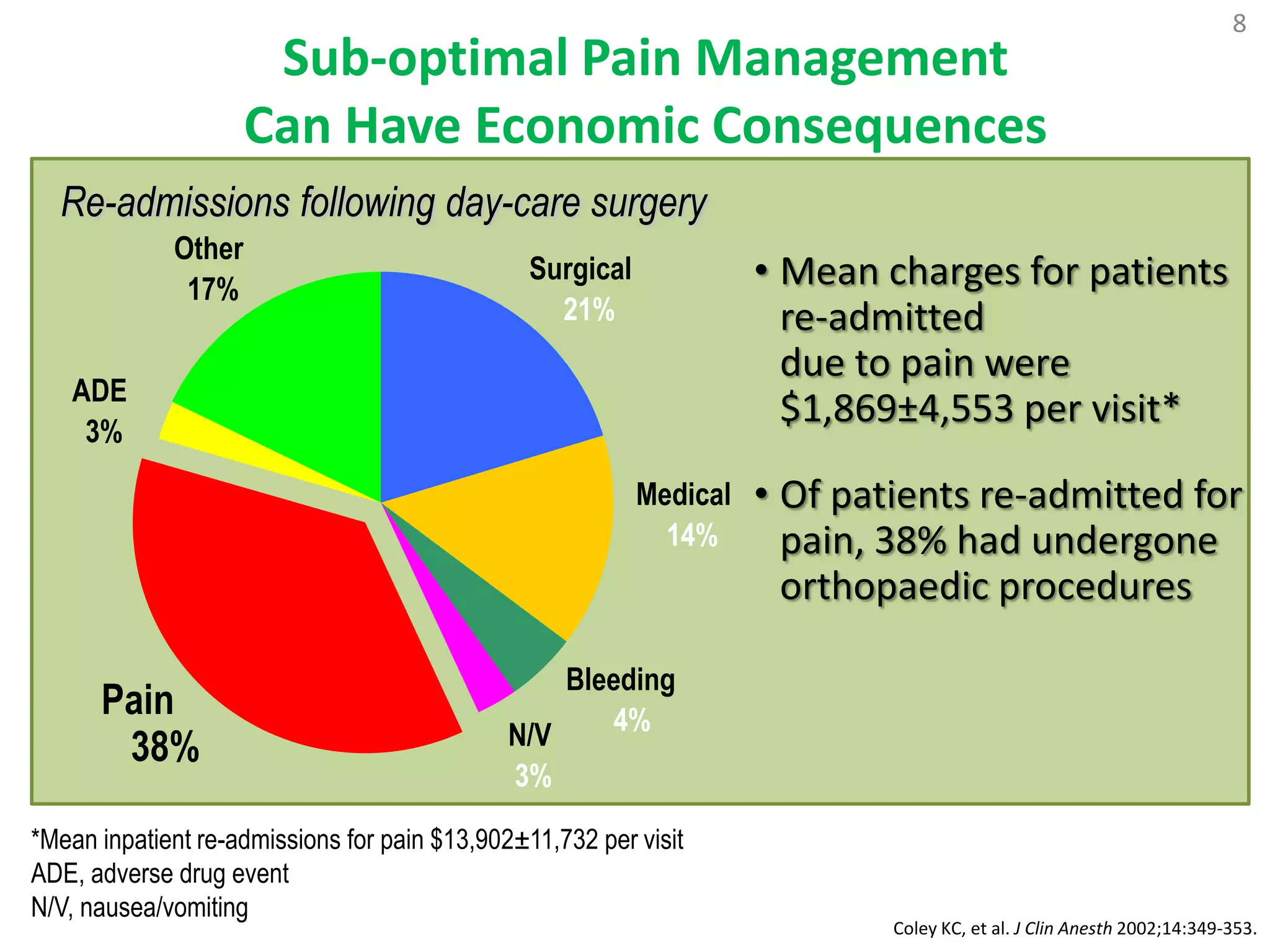
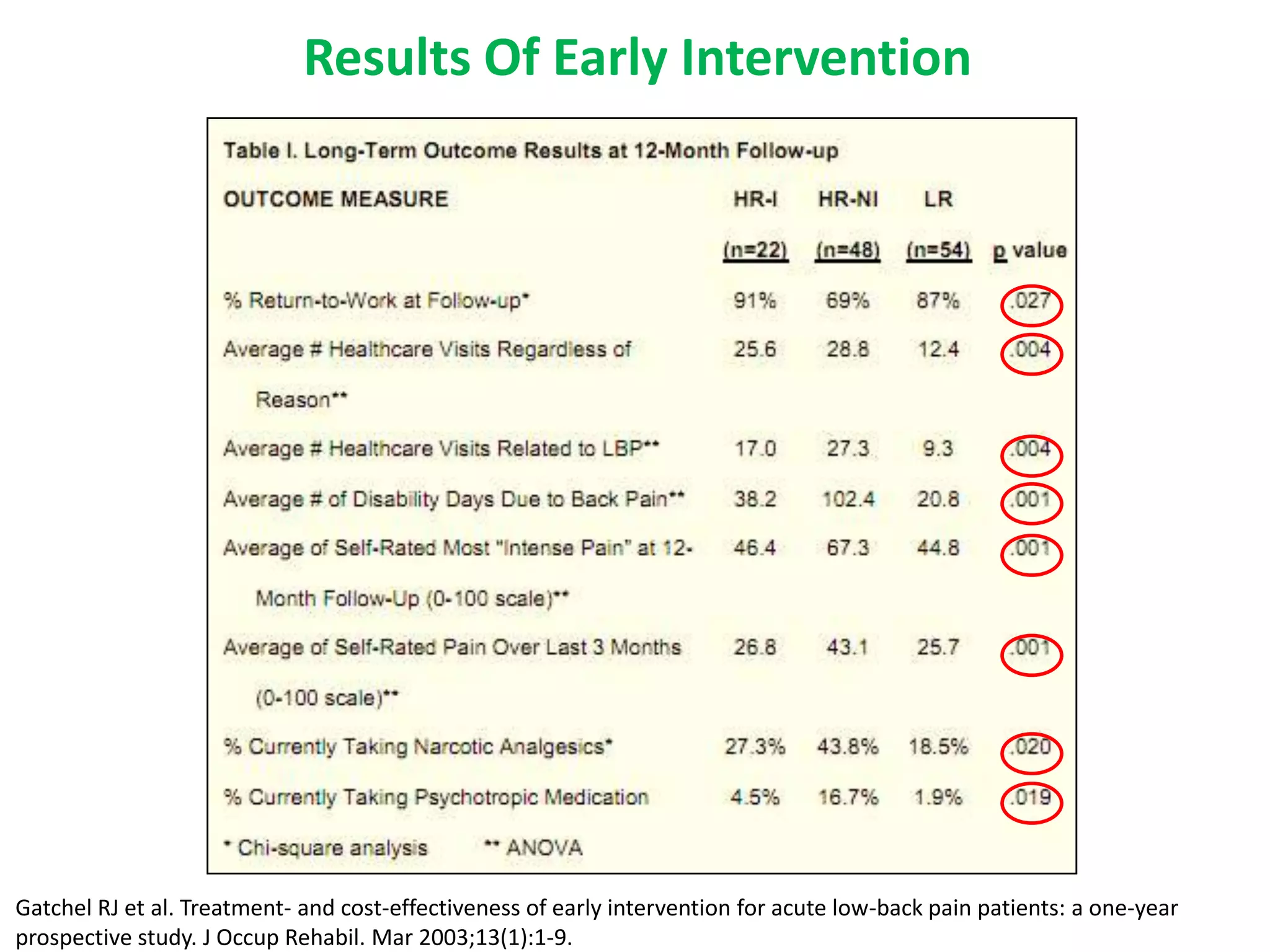
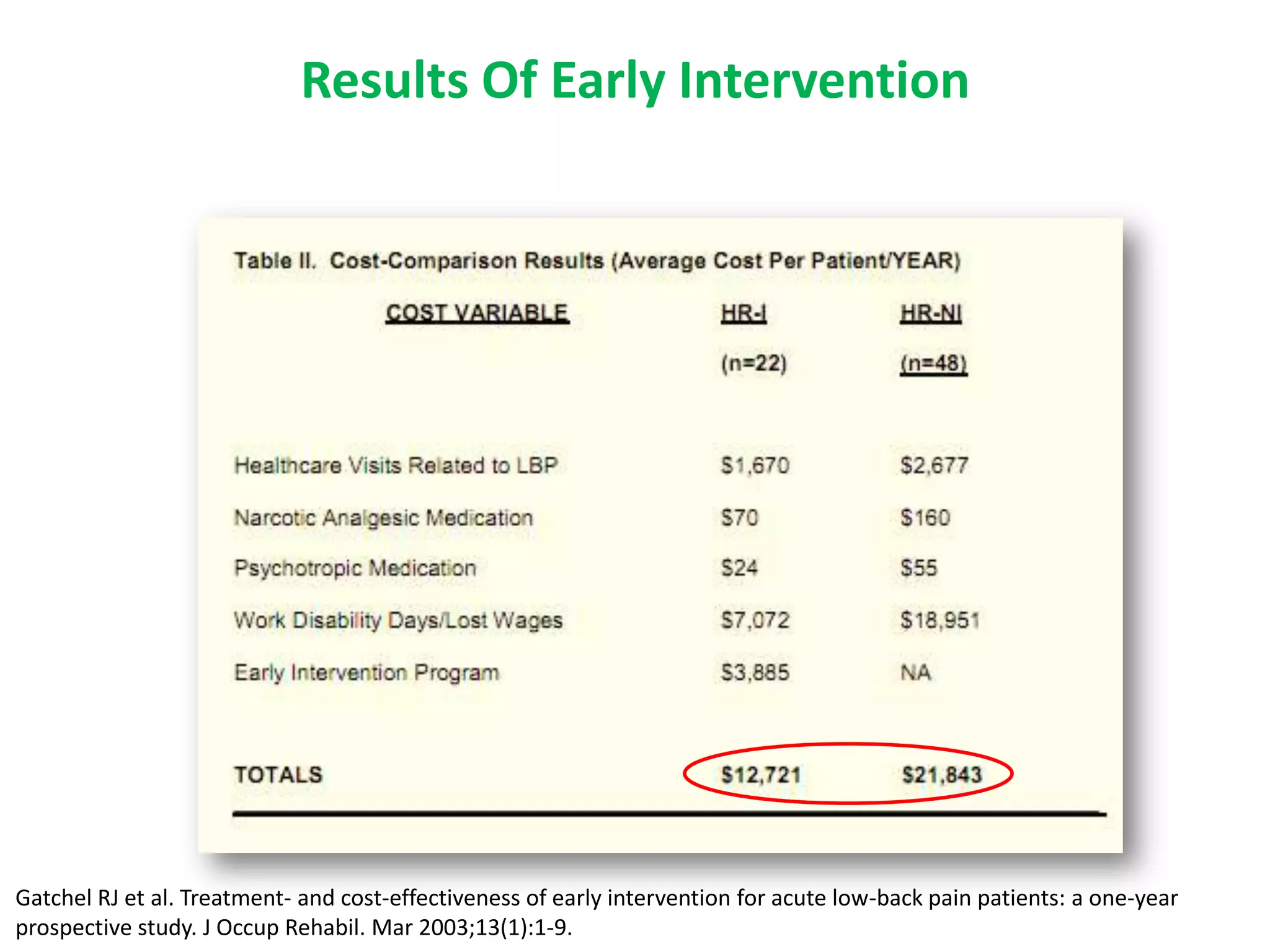
2. Chronic pain poses therapeutic challenges and carries a large economic burden in terms of healthcare costs, lost productivity, and reduced quality of life.
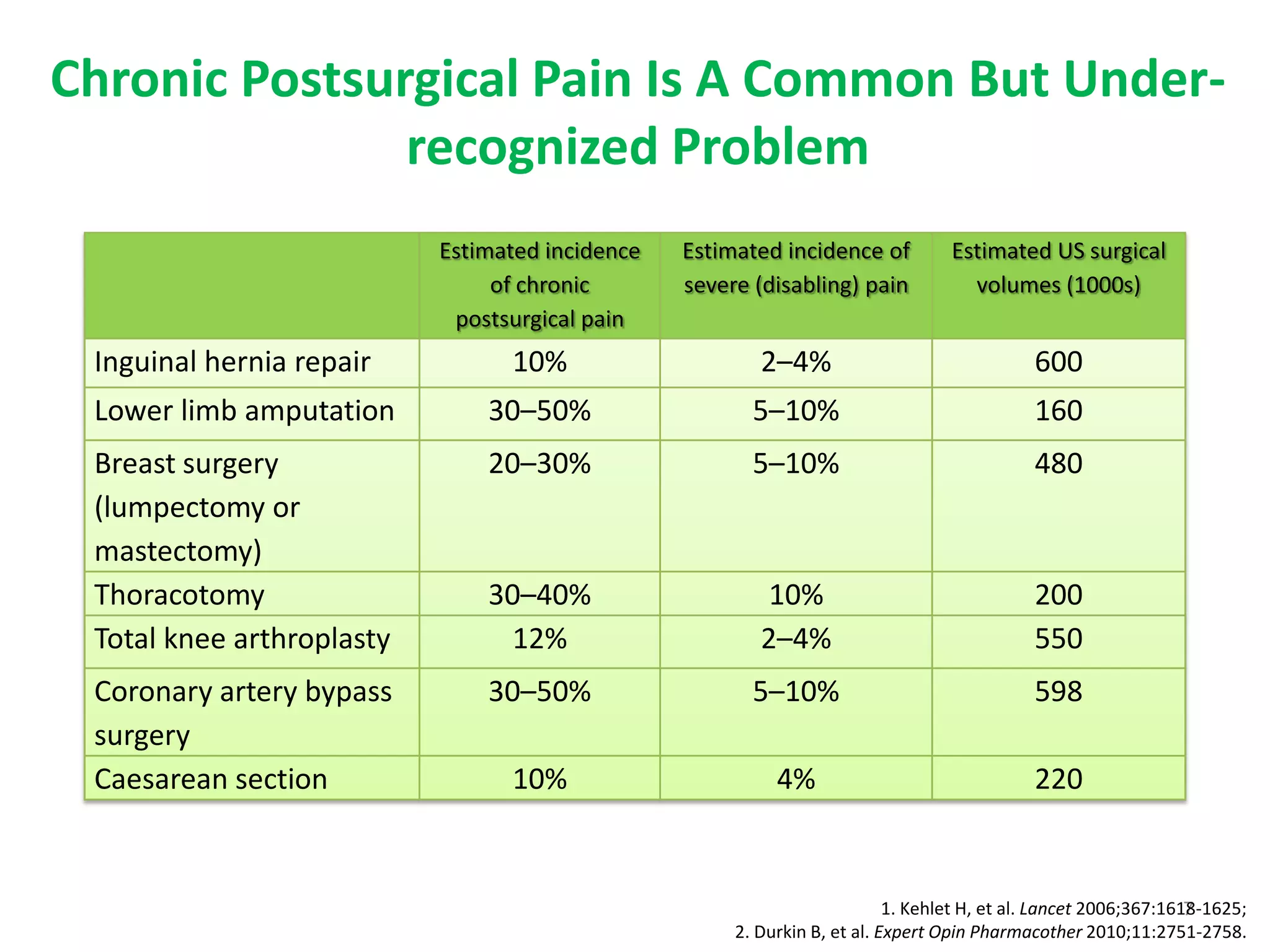
3. Certain surgeries and medical conditions are associated with higher risks of developing chronic postsurgical pain, emphasizing the need for optimal acute pain management after such procedures.