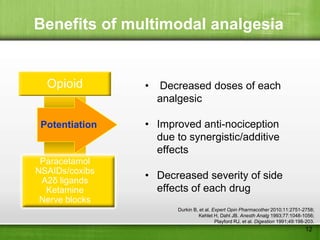
This document discusses managing pain after surgery. It notes that persistent postsurgical pain is often overlooked and can be prevented. A multimodal approach using combinations of analgesics like opioids, NSAIDs, and nerve blocks can improve pain relief while reducing side effects from individual drugs. Identifying patients at risk of chronic pain and using multimodal acute pain management may decrease the risk of acute pain becoming persistent after surgery.