Traumatic Brain Injuryand the
Neurosurgical Patient
Edward J Skicki, DO
Trauma Surgeon
Department of Surgery
Division of Trauma and Acute Care Surgery
Lancaster General Hospital
Edward.Skicki2@pennmedicine.upenn.edu
Last Updated Jan 2024
3.
Disclosure Statement
Ihave no financial interest with manufacturers or any
commercial products related to this presentation
material
Unlabeled/unapproved use of drugs and/or devices will
not be discussed in this presentation
Some of the educational material used in this
presentation is derived from other sources. Resources,
as best as possible, are cited throughout and at the end
of this presentation
4.
Evidence Based Practice
Medicine is an evolving art that practices using
evidence and expert opinion. As a result, this following
presentation is based on evidence based medicine
(with citations included) and experience regarding best
practices.
All evidence based recommendations in this
presentation are up-to-date as of the cited date on the
title slide. Always consult current medical references in
your patient care.
6.
Educational Use Disclaimer
The following is for use in medical education and training.
If reuse qualifies as medical education, material may be
reused under the condition:
– You must cite the author as a reference
– Do not modify the slide content
– If repeating recommendations from published
guidelines, do not modify the recommendation wording
– The author is notified of any erratum so that it may be
corrected
7.
Education Objectives
1. DefineTraumatic Brain Injury (TBI) and Discuss Its
Prevalence
2. Review the Pathophysiology of TBI
3. Review the Symptoms/Manifestations of TBI
4. Review a Focused Evaluation of the TBI Patient
5. Describe the Acute Management of the TBI Patient
6. Describe the Indications for Increased
Monitoring/Consultation for Surgical Intervention
7. Describe the Post-Op Management of the
Neurosurgical Patient
8.
Before We Begin,Some Context:
Aug 8, 2017 – While driving home from work, Dylan was T-boned by
another car at 80mph only a few miles from his home.
The above photograph is not from Dylan’s accident. It and his case are used as part of this didactic reconstruction.
Source: https://triblive.com/local/pittsburgh-allegheny/1-injured-when-car-crashes-into-fence-in-front-of-troy-hill-elementary-school/
9.
He was rushedto a nearby hospital where he was hypotensive with a
small head laceration. He was taken emergently to the OR.
The above photograph is not from Dylan’s accident. It and his case are used as part of this didactic reconstruction.
Source: https://www.inquirer.com/health/a/gun-violence-shot-hospital-emergency-room-trauma-bay-penn-medicine-20190805.html
10.
1
His spleen wasshattered, requiring removal. After resuscitation, he was
brought to the recovery room pending transfer to the ICU.
The above photograph is not from Dylan’s accident. It and his case are used as part of this didactic reconstruction.
Source: https://www.inquirer.com/health/a/gun-violence-shot-hospital-emergency-room-trauma-bay-penn-medicine-20190805.html
11.
1
While in PACU,he did not emerge from anesthesia as expected, so he
was brought the ICU where completion CT scans were done.
The above photograph is not from Dylan’s accident. It and his case are used as part of this didactic reconstruction.
Source: https://www.alfredhealth.org.au/events/basic-assessment-support-in-intensive-care-november-2018/
12.
1
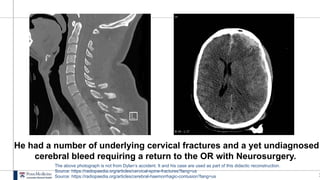
He had anumber of underlying cervical fractures and a yet undiagnosed
cerebral bleed requiring a return to the OR with Neurosurgery.
The above photograph is not from Dylan’s accident. It and his case are used as part of this didactic reconstruction.
Source: https://radiopaedia.org/articles/cervical-spine-fractures?lang=us
Source: https://radiopaedia.org/articles/cerebral-haemorrhagic-contusion?lang=us
13.
1
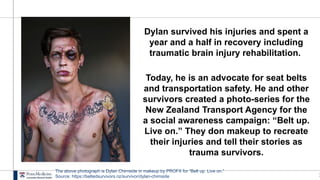
Dylan survived hisinjuries and spent a
year and a half in recovery including
traumatic brain injury rehabilitation.
Today, he is an advocate for seat belts
and transportation safety. He and other
survivors created a photo-series for the
New Zealand Transport Agency for the
a social awareness campaign: “Belt up.
Live on.” They don makeup to recreate
their injuries and tell their stories as
trauma survivors.
The above photograph is Dylan Chirnside in makeup by PROFX for “Belt up. Live on.”
Source: https://beltedsurvivors.nz/survivor/dylan-chirnside
1
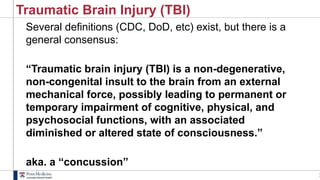
Traumatic Brain Injury(TBI)
Several definitions (CDC, DoD, etc) exist, but there is a
general consensus:
“Traumatic brain injury (TBI) is a non-degenerative,
non-congenital insult to the brain from an external
mechanical force, possibly leading to permanent or
temporary impairment of cognitive, physical, and
psychosocial functions, with an associated
diminished or altered state of consciousness.”
aka. a “concussion”
16.
1
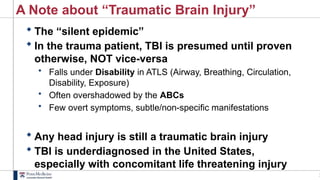
A Note about“Traumatic Brain Injury”
The “silent epidemic”
In the trauma patient, TBI is presumed until proven
otherwise, NOT vice-versa
• Falls under Disability in ATLS (Airway, Breathing, Circulation,
Disability, Exposure)
• Often overshadowed by the ABCs
• Few overt symptoms, subtle/non-specific manifestations
Any head injury is still a traumatic brain injury
TBI is underdiagnosed in the United States,
especially with concomitant life threatening injury
17.
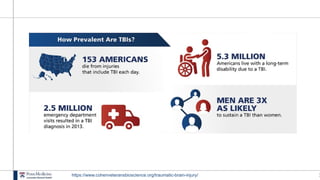
1
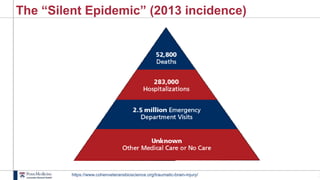
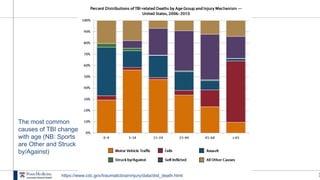
The “Silent Epidemic”(2013 incidence)
https://www.cohenveteransbioscience.org/traumatic-brain-injury/
2
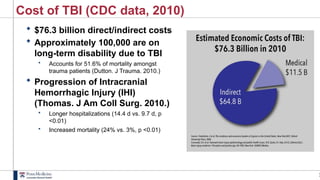
Cost of TBI(CDC data, 2010)
$76.3 billion direct/indirect costs
Approximately 100,000 are on
long-term disability due to TBI
• Accounts for 51.6% of mortality amongst
trauma patients (Dutton. J Trauma. 2010.)
Progression of Intracranial
Hemorrhagic Injury (IHI)
(Thomas. J Am Coll Surg. 2010.)
• Longer hospitalizations (14.4 d vs. 9.7 d, p
<0.01)
• Increased mortality (24% vs. 3%, p <0.01)
2
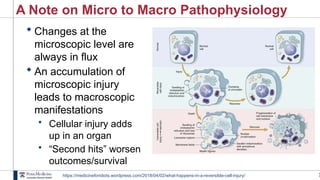
A Note onMicro to Macro Pathophysiology
Changes at the
microscopic level are
always in flux
An accumulation of
microscopic injury
leads to macroscopic
manifestations
• Cellular injury adds
up in an organ
• “Second hits” worsen
outcomes/survival
https://medicineforidiots.wordpress.com/2018/04/02/what-happens-in-a-reversible-cell-injury/
27.
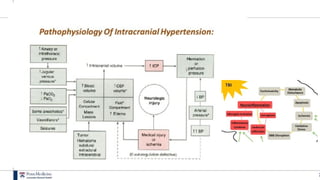
2
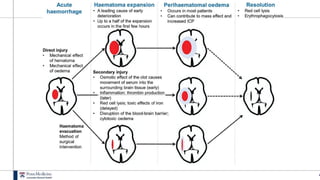
Pathophysiology of Injury
Primary Injury
• Direct trauma and damage to neural tissue
• Irreversible
Secondary Injury
• injury to adjacent tissue due to
– decreased perfusion
– lipid peroxidation
– free radical / cytokines
– cell apoptosis
• Mechanism similar to a stroke from impaired blood flow, compression, and local injury
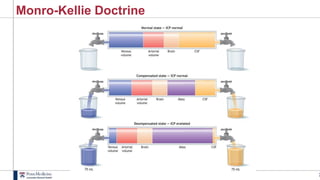
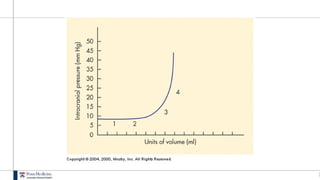
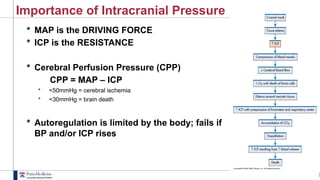
3
Importance of IntracranialPressure
MAP is the DRIVING FORCE
ICP is the RESISTANCE
Cerebral Perfusion Pressure (CPP)
CPP = MAP – ICP
• <50mmHg = cerebral ischemia
• <30mmHg = brain death
Autoregulation is limited by the body; fails if
BP and/or ICP rises
34.
3
Affects of LocalInjury
https://smw.ch/article/doi/smw.2017.14538
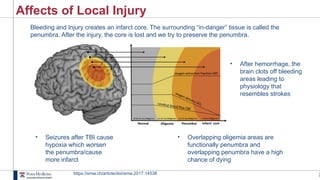
Bleeding and Injury creates an infarct core. The surrounding “in-danger” tissue is called the
penumbra. After the injury, the core is lost and we try to preserve the penumbra.
• Seizures after TBI cause
hypoxia which worsen
the penumbra/cause
more infarct
• Overlapping oligemia areas are
functionally penumbra and
overlapping penumbra have a high
chance of dying
• After hemorrhage, the
brain clots off bleeding
areas leading to
physiology that
resembles strokes
35.
3
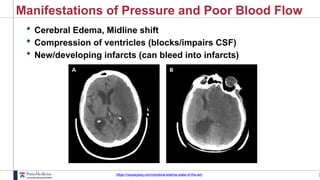
Manifestations of Pressureand Poor Blood Flow
Cerebral Edema, Midline shift
Compression of ventricles (blocks/impairs CSF)
New/developing infarcts (can bleed into infarcts)
https://neupsykey.com/cerebral-edema-state-of-the-art/
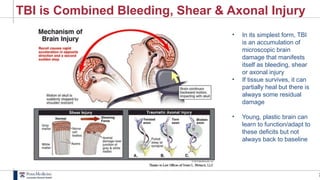
3
TBI is CombinedBleeding, Shear & Axonal Injury
• In its simplest form, TBI
is an accumulation of
microscopic brain
damage that manifests
itself as bleeding, shear
or axonal injury
• If tissue survives, it can
partially heal but there is
always some residual
damage
• Young, plastic brain can
learn to function/adapt to
these deficits but not
always back to baseline
4
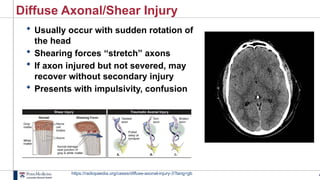
Diffuse Axonal/Shear Injury
Usually occur with sudden rotation of
the head
Shearing forces “stretch” axons
If axon injured but not severed, may
recover without secondary injury
Presents with impulsivity, confusion
https://radiopaedia.org/cases/diffuse-axonal-injury-3?lang=gb
43.
4
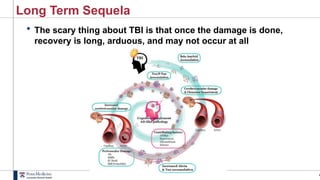
Long Term Sequela
The scary thing about TBI is that once the damage is done,
recovery is long, arduous, and may not occur at all
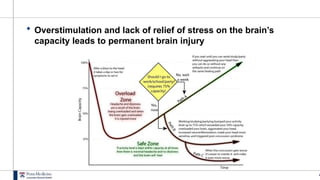
4
Overstimulation andlack of relief of stress on the brain’s
capacity leads to permanent brain injury
46.
4
Repeated/Accumulated Injuries
CHRONIC TRAUMATICENCEPHALOPATHY (CTE)
Progressive degenerative neurological process found in
some athletes who sustain multiple concussions and sub-
concussive blows. This early degenerative process is
characterized by cerebral atrophy and increased levels of tau
protein, as well as cognitive impairment (dementia) and, in
some cases, depression.
LOW-MOD INCIDENCE – HIGH POTENTIAL CHRONIC IMPACT
McKee/Cantu, 2009; Omalu/DeKosky 2005
47.
4
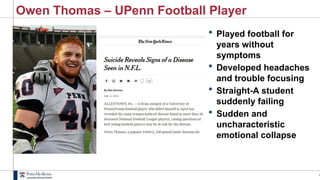
Owen Thomas –UPenn Football Player
Played football for
years without
symptoms
Developed headaches
and trouble focusing
Straight-A student
suddenly failing
Sudden and
uncharacteristic
emotional collapse





































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











