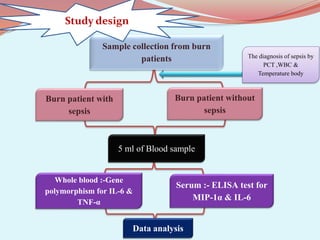
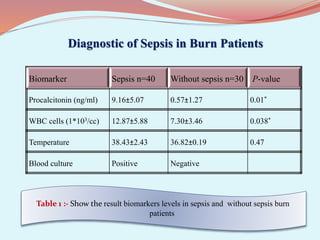
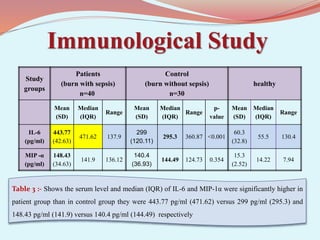
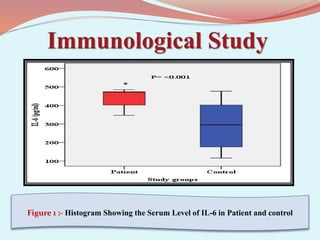
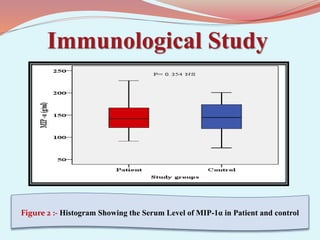
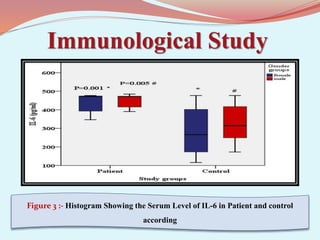
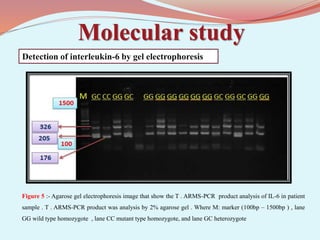
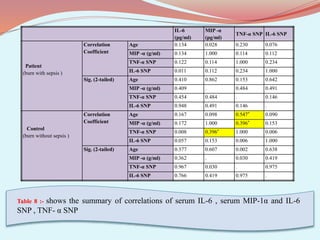
This study aimed to investigate the association between single nucleotide polymorphisms (SNPs) in the IL-6 and TNF-α genes and serum levels of MIP-1α and IL-6 in burn patients who developed sepsis. Blood samples were collected from 40 burn patients with sepsis and 30 burn patients without sepsis. Gene polymorphisms were detected using PCR, and serum cytokine levels were measured using ELISA. The results showed higher serum IL-6 and MIP-1α levels in patients with sepsis compared to controls. No significant differences were found in IL-6 or TNF-α allele frequencies between groups. A correlation was found between IL-6 serum levels and IL-6 genotype in patients with sepsis but not controls.