PREMEDICATIONS
DEFINITION
• Administration ofdrugs before induction of Anaesthesia.
• These medications neither part of the surgical patient’s
usual medical regimen nor are they part of the anaesthetic.
• They are given to reduce anxiety, control of pain, decrease
the risk of aspiration pneumonitis and lower the incidence
of postoperative nausea and vomiting.
.
3.
PRIMARY GOALS
• Anxiolysis& sedation
• Analgesia
• Amnesia
• Increase in gastric fluid pH and decrease in
gastric fluid volume
• Antisialogogue effect
• Decrease SNS reflex response
• Hemodynamic stability
• Decrease in anaesthetic requirement
4.
SECONDARY GOALS
• Facilitationof induction of anaesthesia
• Facilitation of Postoperative analgesia
• Prevention of post operative nausea and vomiting
5.
SEDATION
• A stateof calmness, relaxation or sleepiness caused by
certain drugs.
• Sedation may be used to help relieve anxiety during
medical or surgical procedures.
ANALGESIA
• Insensibility to pain without loss of consciousness.
ANXIOLYSIS
• A level of sedation in which a person is very relaxed and
may be awake. The person is able to answer questions.
6.
SEDOANALGESIA
• Sedoanalgesia isa state which allows
patients to tolerate painful procedures
while maintaining adequate
cardiorespiratory function and the
ability to respond purposefully to verbal
commands and/or tactile stimulation.
7.
Complications from painand anxiety
Stimulation of the autonomic nervous system and release of humoral factors →
increased heart rate, blood pressure, and myocardial oxygen consumption →
myocardial ischemia or infarction
Altered humoral response can lead to hypercoagulability as a result of increased
level of factor VIII, fibrinogen, platelet activity, and inhibition of fibrinolysis
Stress hormones also produce insulin resistance, increased metabolic rate, and
protein catabolism
Immunosuppression with reduction in number and function of lymphocytes and
granulocytes
Psychological disturbances - memories of vivid nightmares, hallucinations, and
paranoid delusions
8.
PREMPTIVE ANALGESIA
Definitionsof Preemptive Analgesia
Three different definitions have been used as the basis
for the recent clinical trials.
Preemptive analgesia has been defined as treatment that:
(1) starts before surgery;
(2) prevents the establishment of central sensitization caused by incisional
injury (covers only the period of surgery);
(3) prevents the establishment of central sensitization caused by incisional
and inflammatory injuries (covers the period of surgery and the initial
postoperative period).
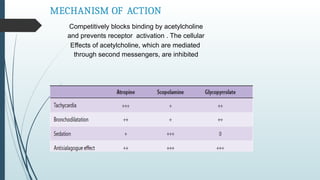
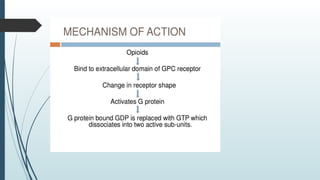
MECHANISM OF ACTION
Competitivelyblocks binding by acetylcholine
and prevents receptor activation . The cellular
Effects of acetylcholine, which are mediated
through second messengers, are inhibited
15.
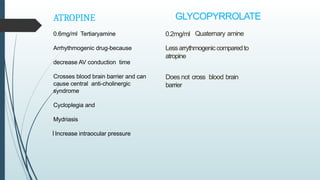
GLYCOPYRROLATE
0.2mg/ml Quaternary amine
Lessarrythmogeniccomparedto
atropine
Doesnot cross blood brain
barrier
ATROPINE
0.6mg/ml Tertiaryamine
Arrhythmogenic drug-because
decrease AV conduction time
Crosses blood brain barrier and can
cause central anti-cholinergic
syndrome
Cycloplegia and
Mydriasis
Increase intraocular pressure
I
16.
ATROPINE
ROUTE OFADMINISTRATION
IM , IV
DOSE 0.02 MG /KG
IM DOSE HALF HOUR BEFORE & IV AT TIME OF INDUCTIOIN
USES
1 AS PREMEDICATION
2 TO TREAT BRADYCARDIA
3 REVERSAL OF NON DEPOLARIZING MUSCLE RELAXANTS
4 OP POISONING
5 FOR FUNDOSCOPY
17.
CONTRA- INDICATIONS
1. Drynessof mouth and throat, difficulty in swalowing.
2. ye: in elderly persons may precipitate acute congestive glaucoma.
Hence, anticholinergics are contraindicated in glaucoma.
3. Difficulty in micturition and urinary retention
4. CNS: Large doses produce restlessness, excitement, delirium and
hallucinations.
5 .CVS: Tachycardia, palpitation and hypotension.
6 . Acute belladonna poisoning: It is more common in children. The
presenting features include fever, dry and flushed skin, photophobia,
blurring of vision, difficulty in micturition, restlessness, excitement,
confusion, disorientation and hallucinations.
Severe poisoning may cause respiratory depression, cardiovascular
colapse, convulsions,coma and death
18.
GLYCOPYRROLATE
Route of administration: i.v,i.m,oralor topical
Dose
0.004 mg/kg i.v.at time of induction &Im at half hour before
induction
Indication:-
Asantisailagogue, intraoperative bradycardia, prevention of
bronchioconstriction
19.
Central anticholinergic syndrome
Cental anticholinergic syndrome
Scopolamine and atropine can cross blood brain barrier when used in high doses,
which can cause central anticholinergic syndrome, it ranges from restlessness to
unconsciousness
Mechanism blockage of muscarinic receptors in the brain
Anti histaminic, antipsycotic, TCA antidepressant posses anticholinergic action can
precipitate central anticholinergic syndrome when combined with other
anticholinergic
METOCLOPRAMIDE
MECHANISM OF ACTION
Metoclopramideacts peripherally as a cholinomimetic (ie, facilitates acetylcholine
transmission at selective muscarinic receptors)and centrally as a dopamine receptor
antagonist
CLINICAL USES
1 As antiemetic
2 GERD
3 To stimulate gastric emptying before GA in emergency
surgeries
22.
SIDE EFFECTS
-Rapid intravenousinjection may cause
abdominal cramping, and metoclopramide is
contraindicated in patients with complete
intestinal obstruction.
-Induce a hypertensive crisis in patients with
pheochromocytoma
-Sedation, nervousness, and extrapyramidal
signs from dopamine antagonism (eg, akathisia)
hence best avoided in parkinson's patient.
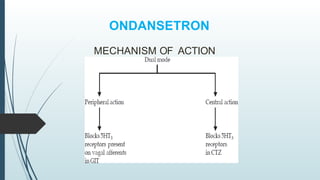
USES:
For prevention andtreatment of
chemotherapy- induced nausea and
vomiting (CINV).
Hyperemesis of pregnancy, postoperative,
post radiation and drug-induced vomiting
but they are ineffective against motion
sickness.
5HT3 receptor antagonist ondansetron can
have analgesic effect in chronic human
Neuropathic Pain (5HT role in progress
and asthma)
26.
DOSAGE
0.06 mg/kg via.i.v. route
0.1 mg/kg via oral route
Dose can be repeated
every 4 -6 hrly
SIDE- EFFECTS
– Constipation
– Headache/flushing
– Elevation of liver
enzymes
PHARMACOKINETICS
It is extensively metabolized in liver.Hepatic
impairment significantly prolongs its half life.No dose
alteration is needed in renal impairment.
27.
H2BLOCKERS
Ranitidine famotidine
MECHANISM OFACTION:
Competitively inhibit histamine binding to H 2 receptors, thereby
reducing gastricacid output and raising gastric pH
ROUTE
: Oral
28.
CLINICAL USES
Reduce theperioperative risk of aspiration pneumonia.
Treatment of peptic duodenal and gastric ulcers, hyper secretory states
(Zollinger–Ellison syndrome), and gastroesophageal reflux disease (GERD).
SIDE EFFECTS
Hypotension
Bradycardia Arrhythmias
MECHANISM OF ACTION
Bindto the proton pump of parietal cells in
the gastric mucosa and inhibit secretion of
hydrogen ions.
CLINICAL USES
Duodenal ulcer,GERD and
Zollinger–Ellison syndrome.
They may promotehealing of
peptic ulcers and erosive GERD more
quickly than H 2 -receptor blockers.
32.
SIDE EFFECTS
-GI system(nausea, abdominal pain, constipation,diarrhea).
- Rare -myalgias, anaphylaxis, angioedema, and severe dermatological
reactions.
-Long-term use-of PPIs has also been associated with gastric
enterochromaffin like cell hyperplasia and an increased risk of
pneumonia secondary to bacterial colonization in the higher-pH
environment
-Omeprazole therapy
-gynecomastia,erectile dysfunction
33.
DRUG INTERACTIONS
PPIs caninterfere with hepatic P-450 enzymes,
potentially decreasing the clearance of diazepam,
warfarin, and phenytoin
.
Concurrent administration
can decrease clopidogrel (Plavix) effectiveness, as
the latter medication is dependent on hepatic
enzymes for activation
34.
MIDAZOLAM
MoA : Occupiesthe benzodiazepenes receptors
which modulate GABA, the major inhibitor
neurotransmitter in the brain.
PHARMACOKINETICS :
Oral bioavailability is 44percent and bio-
availability via IM route is 80 to 100%.
It is 96% plasma protein bound.
Metabolized in liver to hydroxy midazolams 1-
hydroxy midazolam possess 20–30% activity of
the parent compound.
35.
• Clearance 6–11ml/kg/min (most rapid
among all benzodiazepines)
• Elimination half life t½ β = 1.5 to 3.5 hrs.
• 44% Oral
• IV 100%
• 80% IM
• Protein binding(very high) -----Excreted via Kidneys
• Prolongs sedation in renal impairment
36.
PHARMACODYNAMICS
CNS anticonvulsant, hypnotic,anxiolytic, and sedative
action.
-Seizure threshold is raised. Used for
treatment of seizures due to alcohol
withdrawal, LA toxicity and epilepsy.
- Possess centrally acting muscle relaxant
action.
CVS-
Heart rate, cardiac output are well preserved.
Relatively stable hemodynamics due to-slower
onset of action.
RS-
Dose related transient respiratory depression.
Side Effects:
crosses placenta and may depress neonate
37.
It is availableas:
1ml Amp – contains 5mg/ml
5ml vial -contains 1 mg/ml
Clinical Uses :
1. pre-operative medication
2. Intravenous
sedationandamnesia during
a. regional anaesthesia
b. Procedures like endoscopy,
bronchoscopy
c. ICU
d. Postoperatively
3. Induction ofgeneral
anaesthesia.
4.Midazolam nasal spray isused for emergency situations to stop
cluster seizures.
5. IntrathecalMidazolam produces antinocioception and potentiates
theeffect oflocal anaesthetics.
Doses-
Induction-0.05-0.15 mg/kg IV 5 min prior to induction
Maintenance -1.0mcg/kg/min
38.
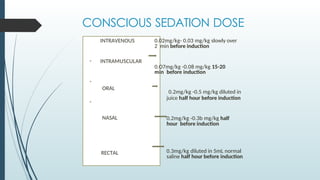
CONSCIOUS SEDATION DOSE
INTRAVENOUS
•INTRAMUSCULAR
•
ORAL
•
NASAL
RECTAL
0.02mg/kg- 0.03 mg/kg slowly over
2 min before induction
0.O7mg/kg -0.08 mg/kg 15-20
min before induction
0.2mg/kg -0.5 mg/kg diluted in
juice half hour before induction
0.2mg/kg -0.3b mg/kg half
hour before induction
0.3mg/kg diluted in 5mL normal
saline half hour before induction
39.
ABSORPTION AND METABOLISM
-More Potent sedative and amnestic than
midazolam and diazepam.
Pharmacokinetics –
Absorption of orally administered lorazepam is rapid,
max blood concentration occurs in 2-4 hr, action
persists for 12-18hrs.
Conjugated with glucuronic acid in the liver to form
pharmacologically inactive metabolites-→ excreted
by kidneys.
Elimination half time- 14hrs
Urinary excretion of lorazepam glucuronide
accounting for more than 80% of injected dose
40.
Pharmacodynamics –
CNS- similarto diazepam
no analgesic properties
RS- stimulant effect on respiration CVS- no
marked change in BP, PR, SVR
Musculoskeletal- muscle relaxant properties.
• Uses- sedation, relief of anxiety.
•also used in ICU sedation Dosage and
administration :
oral (for anxiety) 1-3mg (bd)
• Premedication – recommended oral dose for
preoperative medication is 0.02-0.05 mg/kg
41.
ALPRAZOLAM
- Positive allostericmodulator of GABA-A receptor.
- Triazolobenzodiazepine class
- Taken orally,80% of alprazolam binds to proteins(albumin).
- Metabolized in the liver.
- Dosage- 0.25-1.0mg TDS upto 6mg/day in panic disorder.
- available as- 0.25 mg, 0.5mg, 1 mg, 2mg
- Mainly used as anxiolytic, specifically panic disorder or
generalized anxiety disorder.
- Routinely given 0.5mg night before surgery
42.
Diazepam
• It islipid soluble BZD
• 2cc amp. - 1 cc contains 5 mg
• Dose- 0.2 mg/kg IV slowly diluted
• IM injection- slow and irratic absorption.
• Preservatives- oily injection with preservatives makes IV
injection painful with risk of thrombophlebitis.
44.
Properties
• Hypnotic
• Sedative
•Tranquilizer
• Anxiolytic
• Anticonvulsant
• General skeletal muscle relaxant
• It helps remove muscle spasms
• Produce anterograde amnesia
• It has no analgesia
45.
• Drooping ofeyelids with iv dose- verills sign
• It inhibits the hypoxic drive necessary for respiration. In copd pt
it may lead to resp. Arrest
• Cardiostable - helps to reduce rise in BP due to anxiety
• Crosses placenta and may lead to floppy syndrome
METABOLISM
• Dismethyl diazepam(active)Oxidation, conjugation, dealkylation
• Excreted in urine
46.
USES
• premedication- asanxiolytic
• Induction agent in cardiac pt
• Supplement with regional anaesthesia
• With procedureLA
• Postop along ventilator therapy
• As an anticonvulsant
• In pysch- acute alcohol withdrawal
• Inoculogyric crisis due to phenothiazones,metoclopromide
• To prevent delirium , unpleasant dreams due to ketamine
• Not used in COPD ,myasthenia gravis
47.
Overdose treatment
• Oralcaffeine , sodium benzoate
• Aminophylline 60-125 mg iv slowly
• FLUMAZENIL:-
• Specific antagonism for diazepam
• It has inhibitory effect on BZD receptors
• Dose- 0.2mg to 1 mg ,peak action in 5 min
• Duration of action - 1 to 2 hrs
CLONIDINE
MECHANISM OF ACTION
•Imidazoline derivative acting centrally on alpha-2 agonist.
• Alpha adrenergic agonist in nucleus tractus solitarii which inhibit excitatory cardiovascular neuron
• Reduce sympathetic outflow from cns which decrease BP
• Produce analgesia by affecting dorsal horn neuron
INDICATION
• Antihypertensive
• ADHD
• Tourette syndrome
• Adjunct therapy for cancer related pain
• Hot flushes, prophylaxis of migraine, clonidine suppression test in phaeochromocytoma
• FORMULATION
• Trans dermal patch
• Tablets
• Injection
52.
BIOAVAILIBLITY
RAPIDLY ABSORBED 70– 90%
• 20-40% plasma bound
• Peak plasma level in 60-90 min
• Half life of 12-24 hours
• Elimination half life=9-12hours
• Hypotension after single dose 8hours
• Transdermal patch require 48 hours to achieve therapeutic level
ROUTE OF ADMINISTRATION & DOSE
• ORAL : 4-5µg/kg as preoperatively to reduce
anxiety 300µg orally in pheochromocytoma to
reduce catecholamine release
TRANSDERMAL PATCH: 0.2mg/day applied overnight
day before surgery as well as 72 hours post operatively
• IV/IM/CAUDAL/SPINAL/EPIDURAL ROUTE:
1-2µg/kg as analgesia , 1-1.5µg/kg iv bolus ,1-
2µg/kg/hour infusion
DEXMEDETOMIDINE
MECHANISM OF ACTION
•Selective alpha 2 agonist
• USES & DOSE
• ICU SEDATION: for less than 24 hours in adult
• loading dose: 0.5-1µg/kg over 10-20min followed by 0.1-1µg/kg/hr infusion
• PREMEDICATION: 0.33-0.66µg/kg iv before surgery
• It can also be used intrathecally as neuraxial blockade as well as an adjuvant
in blocks
INDICATION
• Sedation
• Analgesia
• Anxiolysis
• Delirium
SIDE EFFECT
• Hyperglycemia
• Metabolic acidosis
• Agitation
• Hallucination
• Hypotension
• Respiratory depression
• Nausea, vomiting
55.
• CONTRAINDICATION
• Hypersensitivity
•Heart block
• Uncontrolled hypotension
• Acute cerebrovascular condition
• BIOAVAILABILITY
• •94% Plasma protein bound
• Volume of distribution 2-3 L/kg
• Rapid onset of action
• Peak effect with in 15 minutes
• Metabolized by liver
• Eliminated via kidney & feces3-4µ
• Half life about 2-3 hours
56.
Pentazocine
•
• It hasweak µ antagonist and more marked ƙ antagonist actions.
• Profilt of action is similar to morphine; important differences are:
• 1. analgesia caused by pentazocine is primarily spinal(ƙ1) and has a different
character than that caused by morphine.
parenterally 30 mg pentazocine = 10 mg morphine; but the ceilling effect
is lower i.e. at higher doses proportionate increase in analgesia does not
occur.
• 2. Sedation and respiratory depression is 1/3 to 1/2 of morphine and has
lower ceilling effect, does not increase much beyond 60 mg dose.
• 3. Tachycardia and rise in BP are produced at higher doses due to sympathetic
stimulation. This may increase cardiac work; better avoided in coronary
ischemia and myocardial infraction
• Biliary spasm and constipation are less severe.
• Vomiting is less frequent . Other side effects vomiting and lightheadedness.
• Psychomimetic effects can occur.
57.
PHARMACOKINETICS
Oral bioavailabilty is20% due to significant first pass metabolism in liver.
Elimination half life 2 hrs. metabolites excreted mainly via kidneys.
Duration of action of single dose is around
4hrs. oral dose 50-100 mg
im or iv dose 30
onset of action after i.v injection:- 2-3 minutes after
i.m injection:- 20 minutes
intrathecal and epidural also given.
The drug posses irritant property. Local fibrosis occur after repeated I.m or
simultaneous use
DEPENDENCE
The drug has low abuse potential when compared with pure
agonists; however chronic use can lead to physical dependence. It
precipitates withdrawal in morphine dependent subjects.
58.
Actions
CNS – sedation,hypnosis, analgesic
- nausea, vomiting
RS – respiratory depression
CVS – tachycardia, hypertension
- positive inotropic actiondue to
detroisomer
GIT – nausea, vomiting
- not causes constipation.
Less crossingplacenta.
Addiction not seen.
59.
PROMETHAZINE
(PHENARGAN)
• Phenaragan isa first generation antihistamine and antiemetic used to treat allergies, insomnia
and nausea.
• Mechanism of action
• It acts primarily as a strong antagonist of H1 receptor and moderate Ach receptor
antagonist.
PHARMACOKINETICS
• 88% Absorbed but after first pass metabolism reduced to 25% absolute bioavailability.
• Metabolism is by liver glucuronidation and sulfoxidation.
• Elimination half life 10-19 hrs.
• Excretion by kidney and liver
DOSE O.3 – 0.5 mg/kg
Route IV OR IM
2cc ampoule contains
25mg/cc
Given plain or in combination with fortwin , pethidine. Oral
syrup for pediatric 5mg /5cc
60.
Antihistaminic Antitussive
Sedative Antipsychotic
AnticholinergicAntishivering
action
SIDE EFFECTS
It causes hypotension sometime.
Tardive dyskinesia, pseudoparkinsonism, acute dystonia(effects
due to dopamine D2 receptor antagonism)
Confusion in elderly
Drowsiness, dizziness, fatigue, dry mouth, nausea
Respiratory depression in pts under age of two and in those
with severely compromised pulmonary function.
61.
TRICLOFOS
(PEDICLORYL)
• It isa sedative drug used rarely for treating insomnia
• It is a prodrug which is metabolized in the liver into active
drug tricholoroethanol.
• The half life is fairly long and it may cause drowsiness next
day.
Oral tricholorofos syrup (500mg/5ml ) at dose of 50mg /kg if
child cant sleep , it can be repeated 25mg/kg after 30
minutes.
• It may cause liver damage and should not be used for
extended periods
• Side effects
• Headache , rash, dizziness, confusion, confusion,
nightmares,
dependence, nausea, vomiting, abdominal pain
Clinical use
1)1-2 ug/kg: provide analgesia
2)2-20 ug/kg: blunts circulatory response to
Direct laryngoscopy for tracheal intubation
Sudden change in level of surgical stimulation
3)50 ug/kg - produce surgical anaesthesia
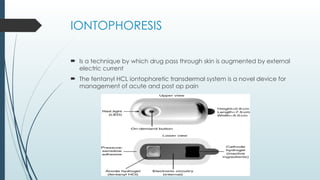
89.
IONTOPHORESIS
Is atechnique by which drug pass through skin is augmented by external
electric current
The fentanyl HCL iontophoretic transdermal system is a novel device for
management of acute and post op pain
OPIOID AGONIST
• INHIBITSASCENDING PAIN PATHWAYS, WHICH CAUSES
ALTERATION IN RESPONSE TO PAIN;
• PRODUCES ANALGESIA (INCREASES PAIN THRESHOLD)
• RESPIRATORY DEPRESSION AND SEDATION
• PHARMACOKINETICS
• HALF LIFE:3-10MIN(RAPID RECOVERY)
• ONSET:1-3 MIN (IV)
• PROTEIN BOUND :70%
• Vd:100ml/kg(small Vd)
• Clearance:40 ml/min/kg(rapid)
• Excretion: Urine
93.
USES
• Induction ofanesthesia
• 0.5-1mcg/kg/min IV
• Maintenance of anesthesia
• 0.25-0.5mcg/kg/min IV; may bolus with 0.5-1 mcg/kg q2-5min
in response to light anesthesia or transient episode of intense
surgical stress
• Prevent laryngoscopy/intubation response
• Conscious analgesia 1mcg/kg IV bolus, followed by 0.05-
0.2mcg/kg/min IV
• Analgesia-IM post op
• 0.025-0.2 mcg/kg/min IV
NALBUPHINE
• Related structurallyto naloxone and oxymorphine.
• Generally considered as µ receptor antagonist and к receptor agonist, with spectrum
of effects that qualitatively resembles that of Pentazocine
• Advantage: Less dysphoria than Pentazocine
• Pharmacological Actions and side effects:
IM dose of 10 mg = 10 mg of morphine with similar onset and duration of
analgesic and subjective effects.
0.2-0.3 mg/ kg IV given before 5 minof induction same as fentanyl
Depresses respiration as much as do equianalgesic dose of morphine,
however nabuphine exhibits a ceiling effect
such as increasing dose beyond 30 mg produce no further respiratory
depression as
well as no further analgesia.
Minimal cardiovascular stimulation:
In contrast to pentazocine and butorphanol, 10 mg nalbuphine given to patients
with stable CAD do not produce
increase in cardiac index, pulmonary arterial pressure or cardiac work, and
systemic
blood pressure is also not
significantly altered. Safe to use in acute MI patients.
Has fewer side effects at 10 mg dose: sedation, headache, sweating are most
96.
BUTRAPHANOL
• It isan opioid agonist antagonist resembles Pentazocine
• It is most used as premedication to blunt laryngoscopic / intubation response, as an Analgesia in
periop and post op period
Mechanism of action Low affinity for µ to produce antagonism
Moderate affinity for к to produce analgesic and anti shivering effects Minimal
affinity for σ, so incidence of dysphoria is low
Availablity 1mg /ml, 2mg/ml ampoule
Nasal spray 10mg /2.5 ml ( each spray consist 1 mg)
Dosage As premedication 1-2 mg IV , 2-3 mg IM
Nasal spray 1mg ( each puff)
Intrathecal 5 -25 mcg /kg
Epidural 1-4mg
Pharmacokinetics Onset 1- 3 min
Half life 2.5 -3.5 hr
Protein bound 70%
Volume of distribution 100ml/kg
Clearance – in urine
97.
BUTORPHANOL
Uses
As premedication toblunt laryngoscopic /intubation response, periop post op Analgesia , As an adjuvant
in Spinal Anesthesia /Epidural, Nasal spray for Migraine pain
S/E:
Sedation, nausea, diaphoresis
Dysphoria is infrequent after buterophanol.
Depression of ventilation is similar to morphine (Above 2.5 – 3
mg dosage , Respirattion depression has ceiling effect )
Increase systemic Blood pressure, pulmonary arterial pressure,
cardiac output.
GI side effects are lower than morphine
Withdrawal syndromes do occur after chronic therapy, but the
symptoms are mild.
98.
Magnesium Sulphate (MgSO4)
•--DOC for preventing and treating convulsions in hypertensive pregnant female.
• Neither an anti epileptic nor an anti hypertensive drug
• Mechanism of action:
i.Blocks Calcium channels, either at motor end plate or at cell membrane reducing calcium
influx.
ii. Decreases Ach release from nerve endings and reduces the motor end plate sensitivity
to
Theraputic Ach.
iii. Blocks NMDA receptors in brain causing cerebral vasodilation.
Before induction:30-50 mg/kg over 10 min with close haemodynamic monitoring
to attenuatestress response to laryngoscopy
Other uses:-Suppression of intubation response
- to reduce fasiculations after succinylcholine
-Antihypertensive
• Level of S.Magnesium : 4-7 mEq/L
• Side Effects:
1st sign of toxicity: Loss of patellar reflex (≥10 mEq/L)
slurring of speech, diaphoresis
Respiratory Depression occurs at ≥12
mEq/L Respiratory arrest occurs at ≥15
mEq/L Cardiac arrest occurs at ≥30 mEq/L
Antidote for Toxicity: Calcium Gluconate IV
(10ml of 10%)
99.
Continue……
Anti Hypertensives (Except
ACEI/ARBs:causesrefractory
Hypotension)
Anti Cholesterol : Statins
Anti Arrythmatics
Alpha blockers
Beta blockers
Nitrate
Digoxin
Anti Epileptics
Anti Anxiety Agents
Anti Depressants
Anti Psychotics
Anti parkinsons
100.
• Anti spasmodics
•Anti histaminics
• Steroids
• Thyroid Drugs
• Anti asthmatics
• Anti gout agents
101.
Drugs to bediscontinued
• OHA
• Insuline
• Anti coagulant agents
• Anti platelets
• ACE inhibitors
• Diuretics
• Lithium
• Combined OC pills
• MAO inhibitors
• NSAIDS
• Herbal medicine
Various preparations ofLignocaine:
• 1% / 2% Lignocaine plain
• 2% Lignocaine+ Adrenalin: 1:80000, 1:200000
• 2% Xylocard
• 5% Lignocaine heavy with dextrose for SA
• 2% Lignocaine jelly
• 4% Lignocaine liquid for topical use
• 4% Lignocaine eye drops
• 5% Lignocaine ointment for anal fissure
• 10% Lignocaine gingival aerosol
• 10% Lignocaine topical spray
• Emla cream (2.5% prilocaine + 2.5% lignocaine)
105.
Mechanism Of Action
•Ionic Migration Theory: blocks the influx of Na+ & K+ through
ion pores of axon membranes,
They stabilize axon membrane.
• Other theory lipid solubility & membrane expansion:
blocking depends on fiber diameter
First autonomic then sensory then motor
Diffusion occurs at axonal membrane at the exposed node of
Ranvier
2-3 nodes at a time
Uses: IV Xylocard2%
• Treat Cardiac Arrhythmia during Anaesthesia: 1-2mg/kg iv bolus
then 4 mg/min for 30 mins then 2 mg/min for 2 hrs then 1
mg/min
• To reduce post op Scoline Pains: 100 mg iv before scoline
• In treatment of intra-arterial spasm due to thiopentone
• Biers block
• Treatment of Status Epilepticus
• To reduce Intra Cranial Pressure
• As Antithrombotic following Arthroplasty
• To prevent Pressure response during laryngoscopy
108.
Uses: As LocalAnaesthetic
• Infiltration Analgesia: Layer wise infiltration into skin
• Field Block for Hernia, Appendix, Breast
• Nerve block/ Conduction Block
• Surface Block for eyes, nose, ears, urethra, meatal surgery,
intra-synovial analgesia
• Bier’s block: IVRA in UL 2-3mg/kg of 1%
Adverse Effects:
• Hypotension
•Arrhythmia
• Neurological effects: contraindicated in epileptic patients
• Hypersensitivity: Mostly due to allergy to preservatives
methyl propylparabene
Showing: dermatitis, rhinitis, asthmatic attack
angioneuratic edema, CVS collapse
• Tachyphylaxis
111.
Toxicity of Lignocaine
•Toxic blood level: 18 microgram/ml
• Seen in patients with: cirrhosis o liver, Renal failure, patients on
cimetidine, beta blocker
• Symptoms: numbness of tongue & mouth, lightheadedness, tinnitus,
slurred speech, restlessness, irrational talking, twitching of facial
muscles, unconsciousness, convulsion, coma, apnea, CVS depression,
hypotension, arrhythmia, arrest
• Treatment: Oxygen, Artificial ventilation in apnea
inj. Thiopentone 200mg IV for convulsion /scoline/diazepam
iv fluids , Vasopressin SOS, iv sodium bicarb SOS
112.
Not to Use:
•In presence of infection, Abscess
• Liver disease
• Malignant hyperthermia
• Lignocaine +Adrenaline avoided locally at end arteries like ear,
nose, skin, penis, fingers
113.
GABAPENTIN
MECHANISM OF ACTION
•Bind to alpha2-delta subunit of calcium channels. This
modulates calcium influx. Without an influx of calcium cells do
not repolarize and the excitatory neurotransmitters release is
inhibited.
• The neurotransmitters inhibited include: glutamate,
norepinephrine, serotonin, dopamine, substance P and
calcitonin gene-related peptide.
• Does not actually bind to GABA or benzo receptors.
114.
Significant
Pharmacokinetics
• Absorption:
• Variable,dose dependent
• Metabolism:
• Not metabolized
• Bioavailability:
• Inversely proportional to dose due to absorption
• Example: 900 mg/day: 60% and 4800 mg/day:
27%
• Excretion:
• Urine as unchanged drug. Proportional to CrCl
• Half life:5-7 h
115.
Uses
:
• Partial seizures/generalizedseizures:300-1200 mg PO TDS
• Neuropathic pain:300-1200 mg PO TDS
• Post herpetic neuralgia:300-600 mg PO TDS
Off label
• Alcohol dependence/withdrawal:300-600 mg PO TDS
• Chronic cough, Hiccups, Hot flashes
• Pain:
• Diabetic neuropathy, Fibromyalgia:400-800 mg PO
TDS, Postoperative pain
• Brachoradial puritis, Uremic puritis
• Restless leg syndrome
• Social anxiety
• 300-1200 mg 1_1.5 hrs before induction
Pregabalin
• Newer Congenerof gabapentin
• Similar mechanism of action
• Same clinical indication in seizure disorder
• Particularly used for neuropathic pain
118.
Significant
pharmacokinetics
• Absorption:
• >90%bioavailability
• Distribution:
• 0% protein bound,
• Metabolism:
• negligible- little drug: drug interactions
• Excretion
• 90% urine as unchanged drug with minor metabolites. Half-life
6.3 hours
119.
Uses:
• Partial Seizures:75 mg BD or 50 mg TDS
• Painful diabetic peripheral neuropathy: 50 mg TDS
• Post herpetic neuralgia: 75-150 mg BD or 50-100 mg TDS
• Fibromyalgia Injury: 75 mg BD
• Spinal cord neuropathies Injury: 75 mg BD
• Off label
• Generalized anxiety
• Hot flashes
• Restless leg
• Social anxiety
Helpful when needing a muscle spasm component
150 mg 1-1.5 hrs before induction of anaesthesia
Contraindications of
Pregabalin &Gabapentin:
• Watch in elderly, renal, alcohol use
• The drug to drug reactions and contraindications are minimal
• Avoid with use of
• CNS Depressants:
• Codeine
• Alcohol
• Hydrocodone/oxycodone/Opioids
• Barbiturates
• Ginko
122.
PREMEDICATION FOR CHILDREN
Thepreoperative period is a stressful time for children specially
in the age group of 2-6 years1
.
It has been observed that anxiety and fear in
children lead to
Preoperatively
o increased catecholamine levels in the
body, thereby leading to, tachycardia,
hypertension, tachypnea
o increased difficulty in gaining intravenous
access,
o separation from parents and
o induction of anaesthesia.
Postoperatively predisposes children to
o sleep disturbances and
o behavioural changes.
123.
An ideal premedicant
relievesanxiety
calms children down
decreases their fear
makes induction smooth
rapid recovery
provides good patient
and parent acceptance
One estimate suggests that 60% of children experience
significant anxiety before anaesthesia induction and
surgery, and this is a global concern for health care
providers2.
Many drugs tried for premedication in children, oral
trichlorofos, opioids, ketamine etc but have side effects
like nausea, vomiting, respiratory depression3.
124.
Intranasal route ofdrug administration is preferred as it is
noninvasive
easily administered
rapid onset
higher bioavailability
Bypass first pass hepatic metabolism
Circumvent blood brain barrier ( via olfactory region of central nervous
system
Well tolerability
No pungency and unpleasant taste
Does not require patient cooperation
avoids problem of volume retention
Examples
midazolam 0.2 mg/kg ( preservative free )
Dexmedetomidine 1 µg/kg ( preservative free )
administered by anaesthesiologist 30 minutes prior to surgery via Mucosal
Atomisation Device intranasally.
125.
Scoring system
Drugacceptance ( compliance score )
Four point sedation score
Parental separation scores
Acceptance to mask (four point score )
126.
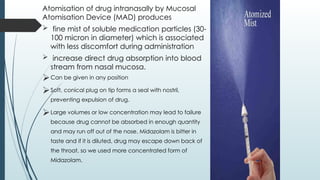
Atomisation of drugintranasally by Mucosal
Atomisation Device (MAD) produces
fine mist of soluble medication particles (30-
100 micron in diameter) which is associated
with less discomfort during administration
increase direct drug absorption into blood
stream from nasal mucosa.
Can be given in any position
Soft, conical plug on tip forms a seal with nostril,
preventing expulsion of drug.
Large volumes or low concentration may lead to failure
because drug cannot be absorbed in enough quantity
and may run off out of the nose. Midazolam is bitter in
taste and if it is diluted, drug may escape down back of
the throat, so we used more concentrated form of
Midazolam.
129.
STAT PEARLS
Themajor objectives of preanesthetic medication are to
(1) allay anxiety,
(2) block autonomic (vagal) reflexes,
(3) reduce airway secretions,
(4) produce amnesia,
(5) provide prophylaxis against pulmonary aspiration of gastric contents,
(6) facilitate the induction of anesthesia, and
(7) if necessary, provide analgesia. Premedication may also decrease the stress
response to anesthesia and prevent cardiac arrhythmias.