Population Health - HEDIS - Health Plan
•
2 likes•601 views

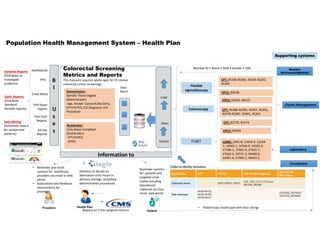
This document describes a population health management system for a health plan. It includes supporting systems like claims management, laboratories, and member services. The system focuses on colorectal cancer screening metrics and uses data from various sources to calculate screening rates. It extracts, cleans, and loads this data into data marts and warehouses. Dashboards, reports, alerts and ad hoc queries are then used to monitor screening rates and identify opportunities for outreach and provider interventions to improve preventive care services.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Population Health - HEDIS - Health Plan
Similar to Population Health - HEDIS - Health Plan (20)
More from CARMEN ALCIVAR
Population Health - HEDIS - Health Plan
- 1. Population Health Management System – Health Plan Supporting systems Member Services(eligibility) Member Services(eligibility) Claims ManagementClaims Management LaboratoryLaboratory Colorectal Screening Metrics and Reports This measure requires adults ages 50-75 receive colorectal cancer screenings. Extract Clean Dashboards LoadStatic Reports (Distribute Standard Periodic reports) Dynamic Reports (Drill down to investigate problems) Data Mining (Automatic search for unexpected patterns) Numerator: Only those Compliant (Numerator) CPT/HCPCS LOINC Numerator: Only those Compliant (Numerator) CPT/HCPCS LOINC Data Marts B I U s e s KPIs Email Alerts Information to Drill Down reports One Click Reports Ad Hoc Reports Denominator: Identify Those Eligible (Denominator) Age, Except: Cancer/Colectomy, CPT/HCPCS, ICD Diagnosis, ICD Procedure Denominator: Identify Those Eligible (Denominator) Age, Except: Cancer/Colectomy, CPT/HCPCS, ICD Diagnosis, ICD Procedure CPT: 44388-44394, 44397, 45355, 45378-45387, 45391, 45392 CPT: 44388-44394, 44397, 45355, 45378-45387, 45391, 45392 LOINC: 2335-8, 12503-9, 12504- 7, 14563-1, 14564-9, 14565-6, 27396-1, 27401-9, 27925-7, 27926-5, 29771-3, 56490-6, 56491-4, 57905-2, 58453-2 LOINC: 2335-8, 12503-9, 12504- 7, 14563-1, 14564-9, 14565-6, 27396-1, 27401-9, 27925-7, 27926-5, 29771-3, 56490-6, 56491-4, 57905-2, 58453-2 HPCS: G0328HPCS: G0328 FOBT Flexible sigmoidoscopy Colonoscopy HPCS: G0105, G0121HPCS: G0105, G0121 HPCS: G0104HPCS: G0104 CPT: 45330-45335, 45337-45342, 45345 CPT: 45330-45335, 45337-45342, 45345 CPT: 82270, 82274CPT: 82270, 82274 Member ID • Name • DOB • Gender • SSN Providers Health Plan Patient • Reminder and recall systems for healthcare providers via email or web portal • Assessment and feedback interventions for providers. Reminder systems for patients and targeted small media including educational materials via mail, email, web portal Reports on 5 star program metrics EnrollmentEnrollment • Patient buys health plan with best ratings Statistics to decide on alternative clinic hours or delivery settings, simplified administrative procedures
- 2. References Sources: • https://www.google.com/imgres?imgurl=http://practicalanalytics.files.wordpress.com/2013/07/healthvaluechain.png&imgrefurl= http://practicalanalytics.co/2013/07/15/informatics-or-analytics-understanding-healthcare-provider-use- cases/&h=612&w=1023&tbnid=C83W5EDinr4CdM:&docid=bceW7m0m7yh4JM&ei=-drpVomhE4bW- QGc3KmADw&tbm=isch&ved=0ahUKEwjJgZvMncbLAhUGaz4KHRxuCvAQMwgnKAowCg&biw=1366&bih=667 • https://www.google.com/imgres?imgurl=https://www.healthcatalyst.com/wp-content/uploads/2013/07/enterpruse-data-model- grphic.png&imgrefurl=https://www.healthcatalyst.com/best-healthcare-data-warehouse- model&h=732&w=975&tbnid=d5RUhcbuBmfimM:&docid=KXbM8E7SBuassM&ei=-drpVomhE4bW- QGc3KmADw&tbm=isch&ved=0ahUKEwjJgZvMncbLAhUGaz4KHRxuCvAQMwhDKBowGg#h=732&imgdii=d5RUhcbuBmfimM%3A% 3Bd5RUhcbuBmfimM%3A%3Bj30fAU63iplVUM%3A&w=975 • https://www.bcbsnc.com/assets/providers/public/pdfs/u9209m_hedis_provider_tool_for_colorectal_cancer_screening.pdfhttps:/ /www.google.com/imgres?imgurl=http://image.slidesharecdn.com/healthcarepayermedicalinformaticsandanalytics- 140714155347-phpapp01/95/healthcare-payer-medical-informatics-and-analytics-30- 638.jpg%253Fcb%253D1405353445&imgrefurl=http://www.slideshare.net/frankfangwang/healthcare-payer-medical-informatics- and-analytics&h=479&w=638&tbnid=iYCwbNES47gKRM:&docid=HoRKPe2IhWI9UM&ei=-drpVomhE4bW- QGc3KmADw&tbm=isch&ved=0ahUKEwjJgZvMncbLAhUGaz4KHRxuCvAQMwgfKAIwAg#h=479&w=638 • https://www.google.com/search?espv=2&biw=1366&bih=667&tbm=isch&sa=1&q=dashboards+health+care&oq=dashboards+hea lth+care&gs_l=img.3...36026.39556.0.39658.0.0.0.0.0.0.0.0..0.0....0...1c.1.64.img..0.0.0.2gqWhPkjmYI • http://www.cdc.gov/pcd/issues/2013/13_0180.htm • http://www.hrsa.gov/quality/toolbox/measures/colorectalcancer/part4.html • Presentation class 12 Data Management