
Recommended
More Related Content
Similar to POLY ARTERITIS NODOSA POLY ARTERITIS NODOSA
Similar to POLY ARTERITIS NODOSA POLY ARTERITIS NODOSA (20)
More from pranavkohli8
More from pranavkohli8 (13)
Recently uploaded
Recently uploaded (20)
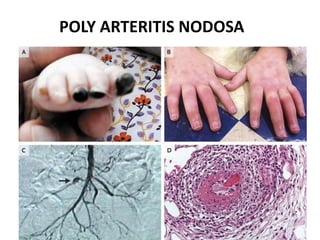
POLY ARTERITIS NODOSA POLY ARTERITIS NODOSA
- 2. CLASSIC POLYARTERITIS NODOSA • It involves purely medium vessel vasculities • It is a systemic vasculitis characterized by necrotizing inflammatory lesions ,preferentially at vessel bifurcation resulting in microaneyrysm formation,aneurysmal rupture with hemorrhage,thrombosis,and,consequently,organ ischemia or infarction. EPIDEMIOLOGY • PAN is a rare disorder • With an incidence of about 3 to 4.5 cases per 100,000 population anually. • M=F • Seen in 4th to 6th decade also seen in young patients
- 3. PATHOPHYSIOLOGY • The exact mechanism is not known • Vascular lesions in medium-sized muscular arteries occur mainly at bifurcations and branch points . • Inflammation may start in the vessel intima and progress to include the entire arterial wall destroying the internal and external elastic lamina resulting in fibrinoid necrosis. • Aneurysm develop in the weakened vessel,carrying a subsequent risk for rupture and hemorrhage • Thrombi may develop at the site of lesions • As lesion progress,proliferation of the intima or media may result in obstruction and subsequent tissue ischemia or infarction • It spares the large vessels [the aorta and its major branches],the smallest vessels {capillaries andsmall arterioles},and the venous system • Loss of function of mutations in CER1, the gene that encodes adenosine deaminase 2 (ADA2),have ben associated with spectrum of vascular and inflammatory phenotypes that includes PAN.
- 4. HISTOLOGY • Fibrinoid necrosis in the vessel wall is present • Transmural segmental necrotizing inflammation.All stages of inflammation can be seen in a single vessel
- 5. ETIOLOGY • Hepatitis B and PAN • Hepaititis B virus {HBV} infection is strongly linked with PAN. Evidence for immune complex-induced disease is confined to HBV-related PAN;the role of immune complexes in non-HBV-related PAN remains unclear. • Impaired function of endothelial cells may be part of idiopathic PAN or a consequence of it,in HBV-PAN virus replication may directly injure the vessel wall. • Endothelial dysfunction can perpetuate the inflammation through cytokine and adhesion molecule production • There is 30:1 rule in PAN and HBV
- 6. IMPORTANT FEATURES • PAN do not present as 1. petechiae 2. Purpura 3. Vesicle 4. Bulla • But presents as 1. Nodules 2. Deep ulcers 3. gangrene
- 7. • Glomerular capillaries and DAH are not manifested instead,involvement of bronchial arteries can cause hemoptysis • No antibodies in PAN. ANCA negative • Immune complexes and granulomas are absent • It has transmural involvement with necrotising vasculitis,fibrinoid necrosis,neutrophilic infiltration. • It is focal and segmental • BAD prognosis commonly assosiated with Hep B, hairy cell leukemia, and ADA-2 deficiency
- 8. Other Associations • Varicella-zoster virus • Parvovirus B-19 • Cytomegalovirus • Human T-cell leukemia virus • Rhematoid arthritis and sjogren syndrome have been also associated with PAN
- 9. CLINICAL FEATURES • PAN is an acute multisystem disease with a relatively short prodrome (ie,weeks to months) • Constitutional and musculoskeletal system sumptoms of PAN includes • Fever • Malaise • Fatigue • Anorexia and weight loss • Myalgia • Arthralgia in large joints or less commonly arthritis
- 10. RENAL SYMPTOMS • About 60% of patients have renal involvment • Flank pain may be present • Ischemic changes in the glomeruli and renal artery vasculities can cause renal failure,hypertension or both • A small % of patients may require dialysis • SYMPTOMS • Hypertension • Costophrenic tenderness • Retroperitoneal or intraperitonial hemorrhage
- 11. CUTANEOUS SYMPTOMS • Dermatalogic symptoms are very common in PAN and about 405 of patients manifest with skin lesions including • Gangrene,nodules,cutaneous infarcts,livido reticularis • Livedo reticularis that does not blanch with active pressure • Ulcerations-Especially on lower extremities near the malleoli and calf
- 17. CNS SYMPTOMS • Cerebral arteritis ,which can cause cerebral ischemia and sub-archanoid heamorrage late presentation usually in second to third year of vasculitis • Acute or sub-acute myelopathy with paraparesis can occur at any cord level • Mononeuritis multiplex –infarction of (radial,ulnar,peroneal,sural).although nerve involvment is initially asymmetrical,the development of additional nerve lesions can cause the clinical picture to resemble symmetrical polyneurophathy • Rare less than 10% encephalopathy focal defecits strokes,seizures,and sometimes brain haemorrages PERIPHERAL NERVOUS SYSTEM SYMPTOMS : 1. Distal neurophathy 2. Cutaneous neurophathy GASTROINTESTINAL SYMPTOMS : • Abdominal pain which may be post prandial • Nausea and vomiting with or without GI bleeding • Rare and more serious complications are • Bowel infarction and perforation • Cholecystitis • Hepatic infarction • Pancreatic infarction
- 18. CARDIAC SYMPTOMS • Hypertension • Tachycardia out of proportion to fever • Pericardial friction rub • Arrythmias • Congestive heart failure OPTHALMOLOGIC SYMPTOMS • Retinal vasculitis • Retinal detachment • Cotton wool spots
- 19. DIFFERENTIAL DIAGNOSIS • Antiphospholipid syndrome • Eosinophilic granulomatasis polyangitis (churg-strauss syndrome) • Granulomatosis with polyangiitis (wegener granulomatosis) • Henoch-schonlein purpura • Small vessel vasculitis • Microscopic polyangitis
- 21. DIAGNOSIS • LAB findings ain PAN are nonspecific but can help to establish the systemic nature of the disease • Elevated ESR/C-reactive protein .These markers may be useful in evaluating some patients for active disease but do not correlate with activity in all patients • Thrombocytosis • Hepatitis B surface antigen and hepatitis C serologies • Elevated creatinine levels • Mild proteinuria • Elevated liver enzymes • Hypergammaglobulinemia • Decreased levels of complements (ie,C3,C4) • MR/CT ANGIOGRAM : microaneurysms are seen • DANGER SIGNS : abdominal pain/renal and CNS involvement
- 23. MANAGEMENT OF THE PATIENT • INVESTIGATIONS • MR-angiography • 5 FACTOR SCORE : CNS,CVS,GIT,proteinuria,sr.creatinine • ADA 2 in children : deficiency closely resembles PAN. Pure cutaneous involvement with small arteries and arterioles sparing the venules.
- 25. ACR CRITERIA PAN : 1. Weight loss >4kg 2. Livido reticularis 3. Testicular pain 4. Mononeurophathy 5. Systemic hypertension ,diastolic BP > 90 6. HbsAg 7. Aneurysm on arteriogram 8. BIOPSY: necrotising vasculitis with granulocyte and monocytes in arterial wall 9. Increase in blood urea or creatinine levels which is not related with dehydration or obstruction
- 26. TREATMENT • Immunosuppression continous to be standard therapy for PAN • Corticosteroids and cyclophosmide can prolong survival for patients with idiopathic PAN • For non-hep B patients : steroids and cyclophosphamide(response is poor) • For hep-B patients : steroids+Antiviral and plasmopheresis (PLEX). (Response is poor ) • Antiviral agents like tenofovir alaenamide is used.
- 27. PROGNOSIS Idiopsthic (non-HBV- related PAN) : • Recovery from neurological defecits due to PAN can take upto 18 months. CNS involvement carries a worse prognosis than does peripheral nerve involvement • The prognosis is markedly worse in patients with acute abdominal syndromes charecterized by extensive bowel involvement • Multiple perforations may be found,relapse are common,and the post operative course is complicated by infections and delayed healing. • The prognosisis better in patients with cutaneous PAN without systemic involvement.This disease is benign and tends to relapse HBV-related PAN : • Patients who seroconvert usually recover • Once HB-PAN goes into remission, the risk of recurrence is very low HCV-related PAN • One study found that in patients with HCV-related vasculitis, HCV PAN exhibits a more severe clinical presentation but a higher rate of clinical remission.
- 28. THANK YOU