1) The study found that placebo analgesia activates the endogenous opioid system by examining the effects of naloxone on placebo responses.
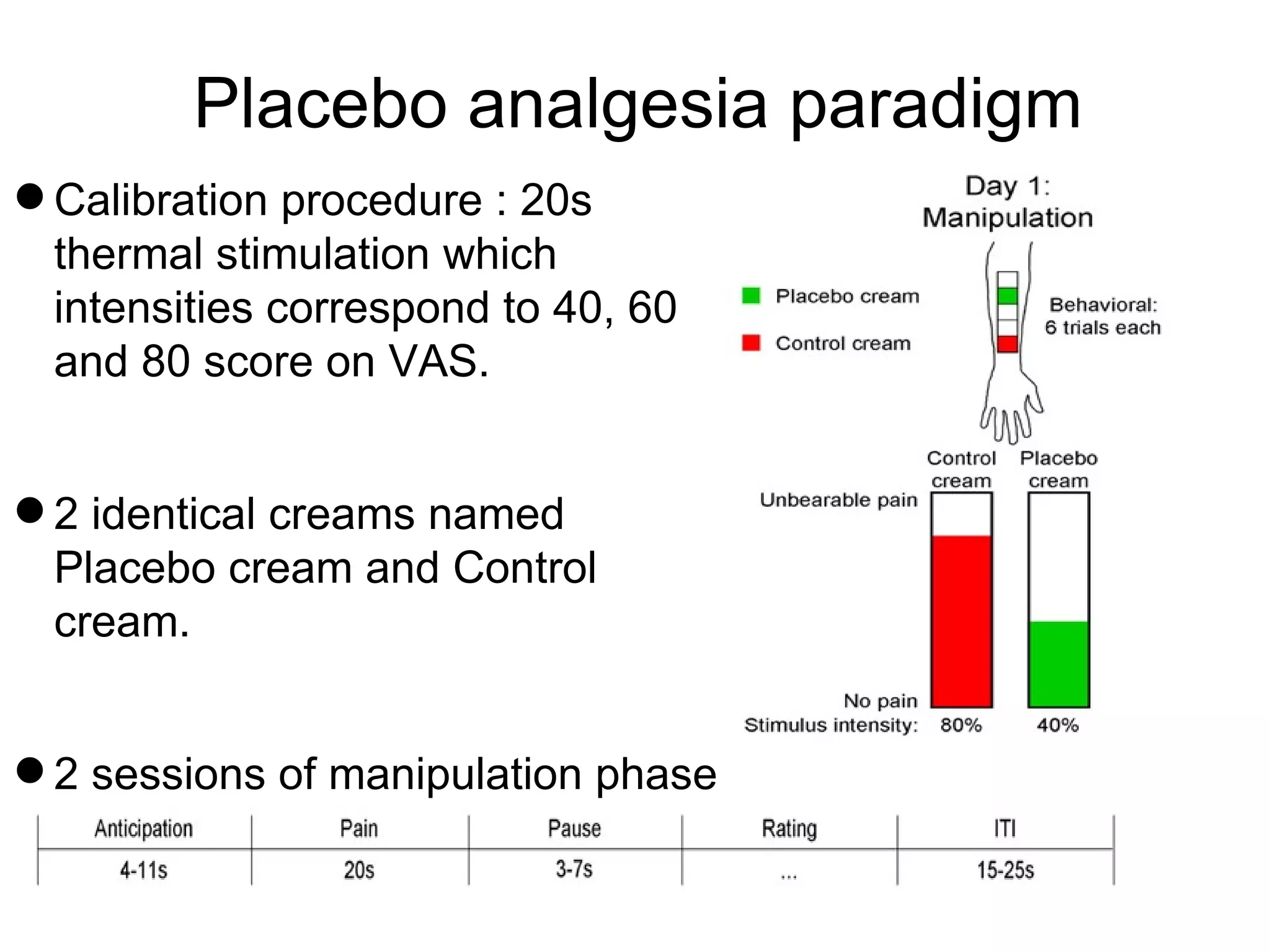
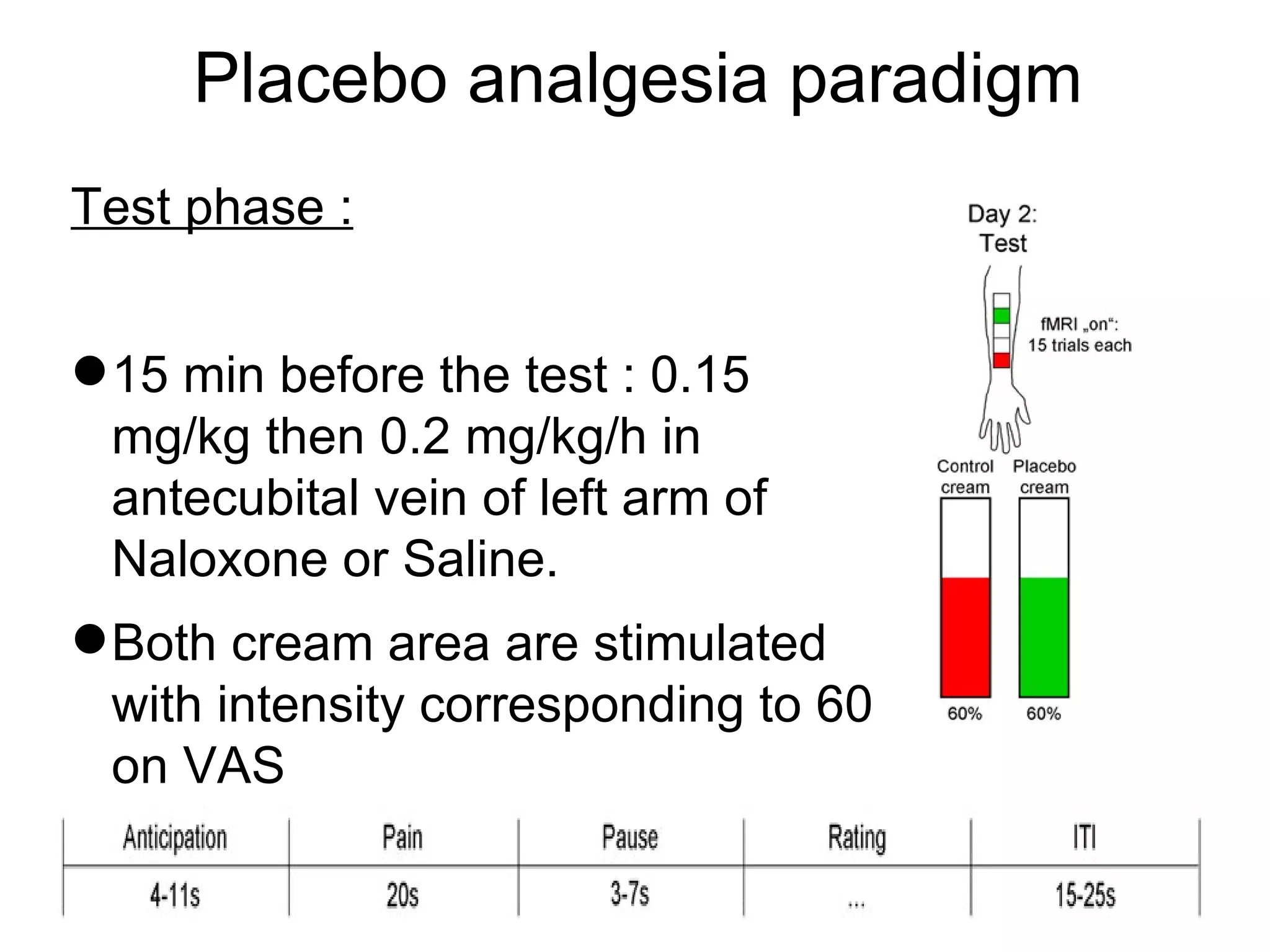
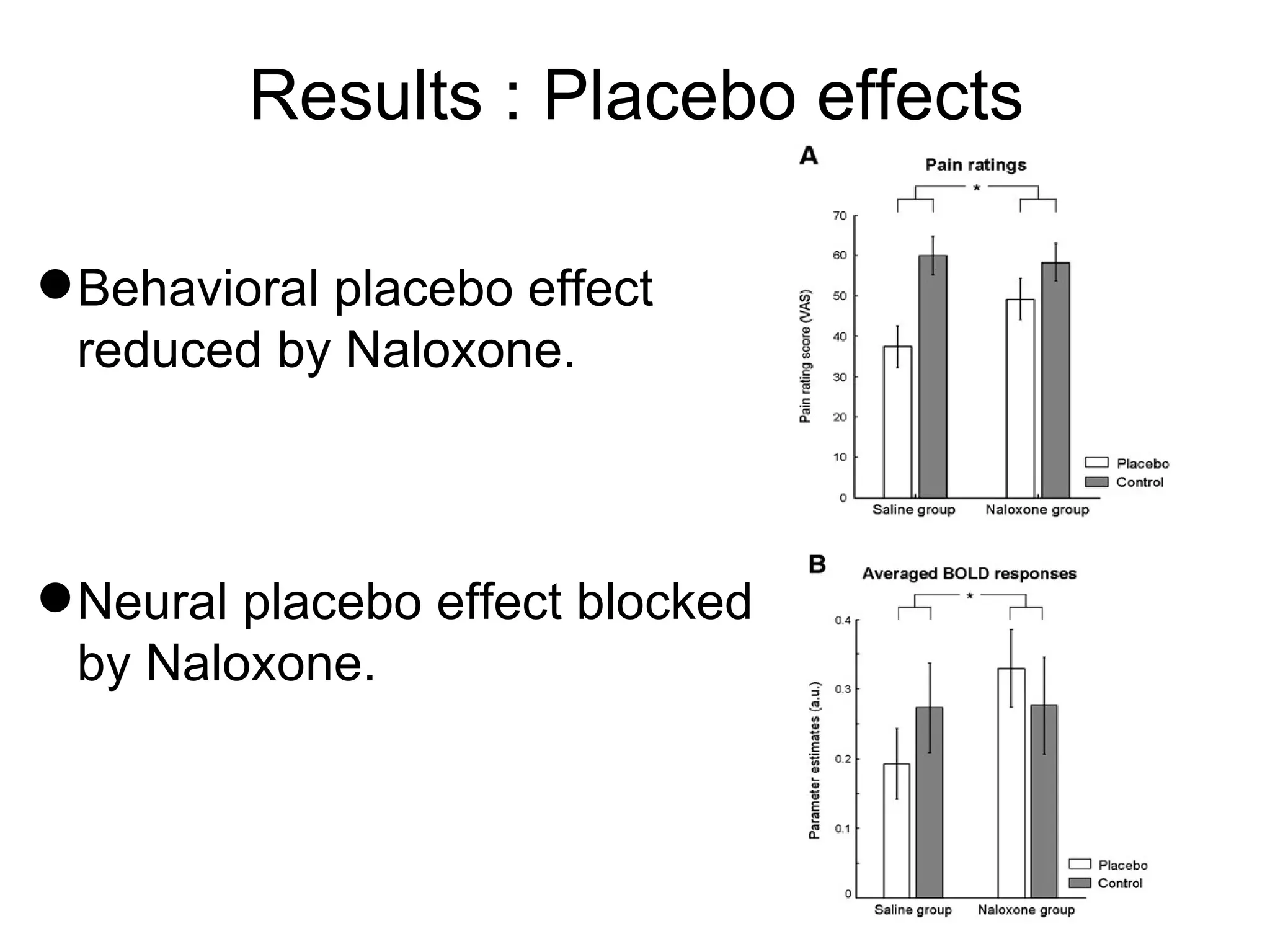
2) Subjects received either naloxone or saline before a thermal pain test, where one area was treated with a placebo cream. Naloxone reduced both behavioral and neural placebo effects.
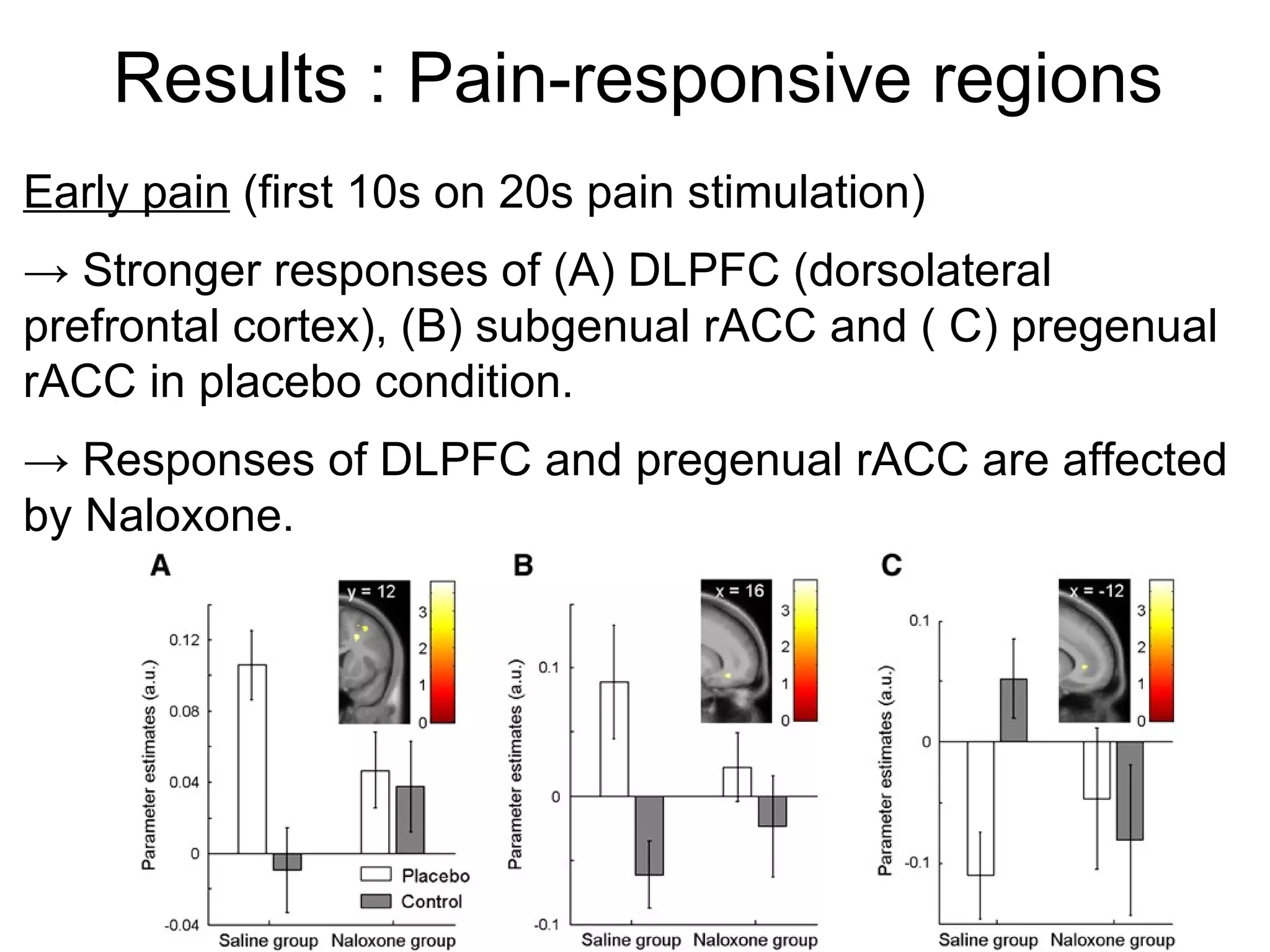
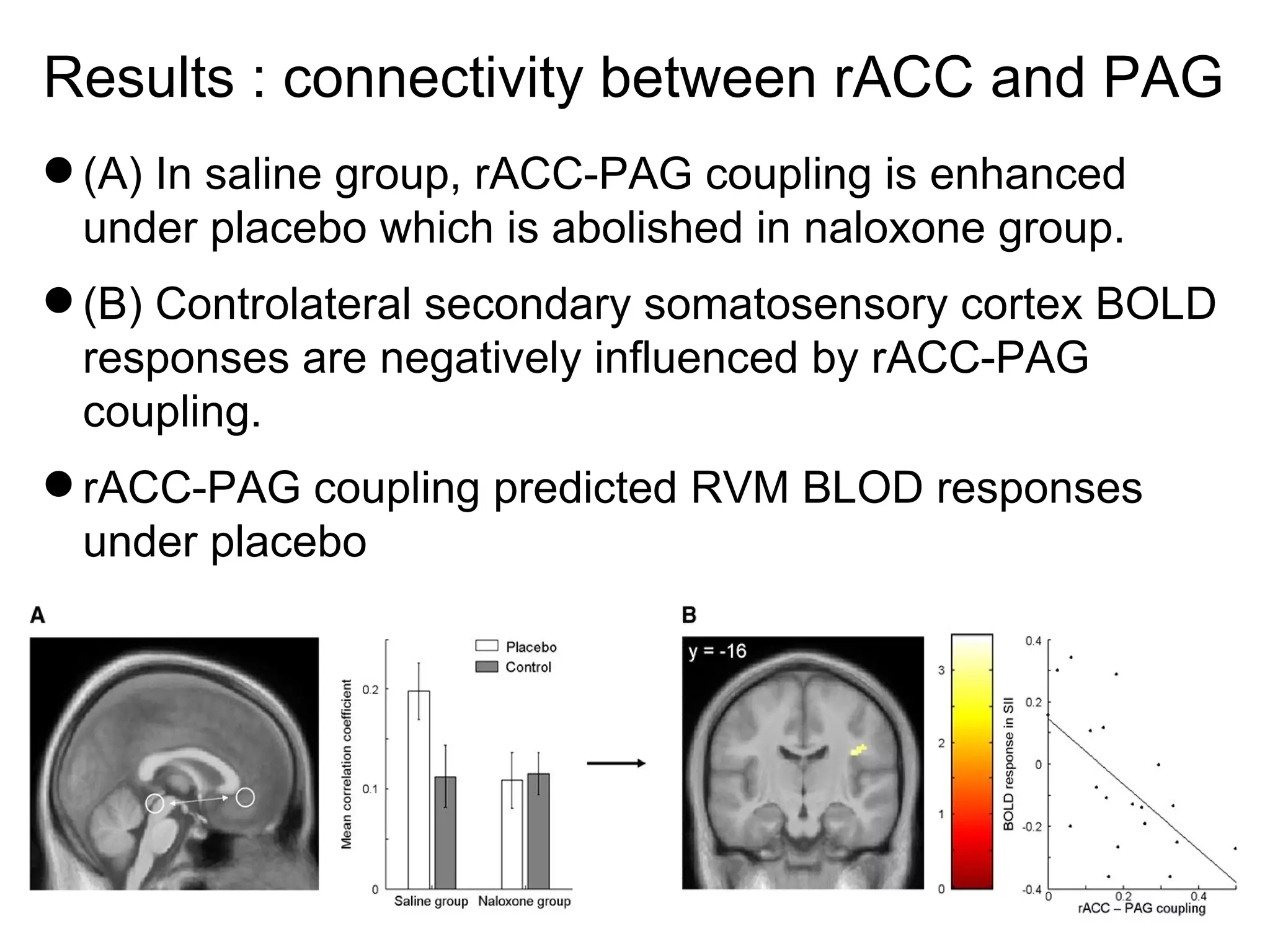
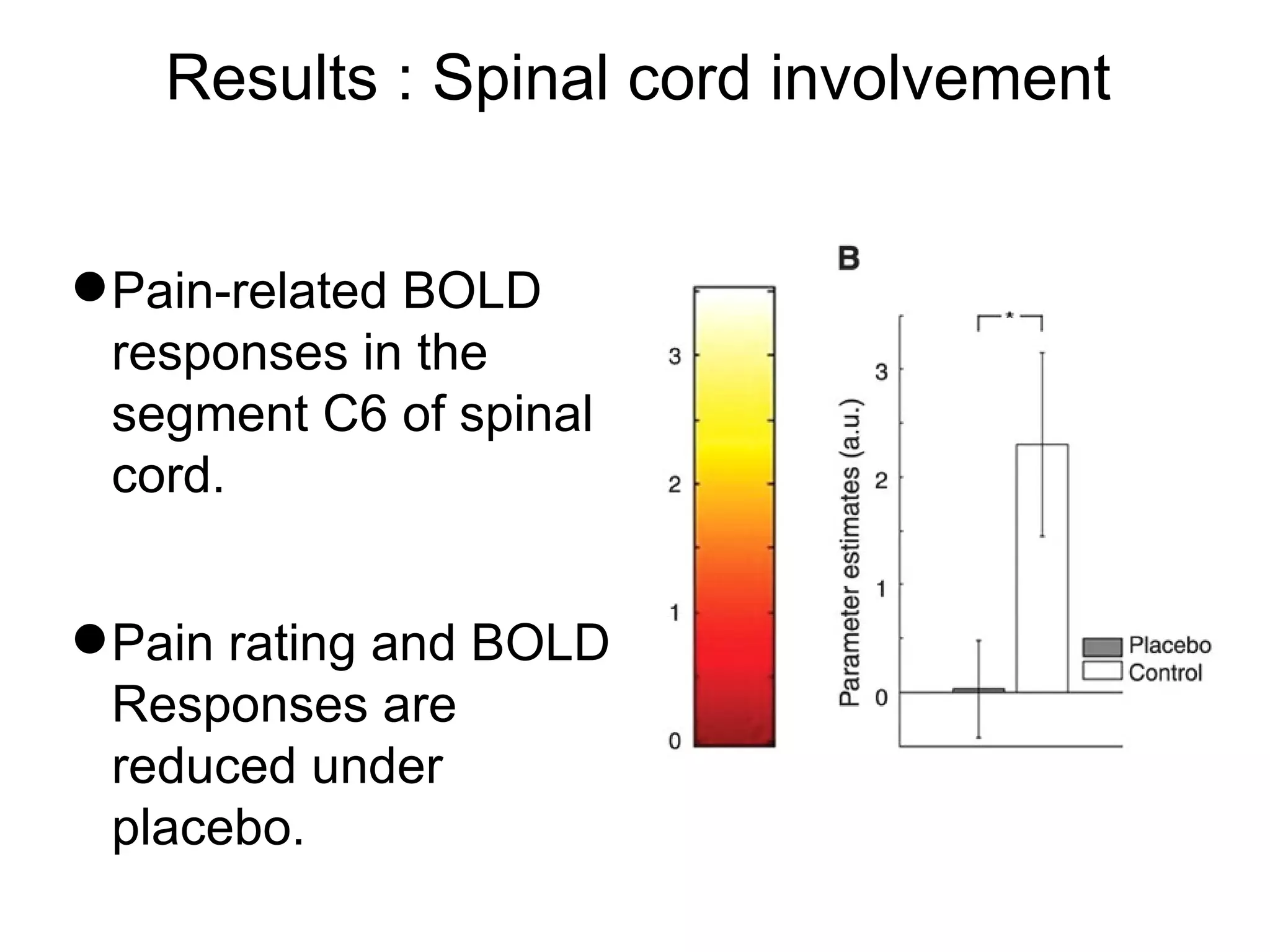
3) Brain regions involved in pain processing like the rACC, PAG, and RVM showed stronger responses to placebo that were blocked by naloxone, indicating the role of endogenous opioids. The main pathway of placebo analgesia involves PAG -> RVM -> spinal cord.