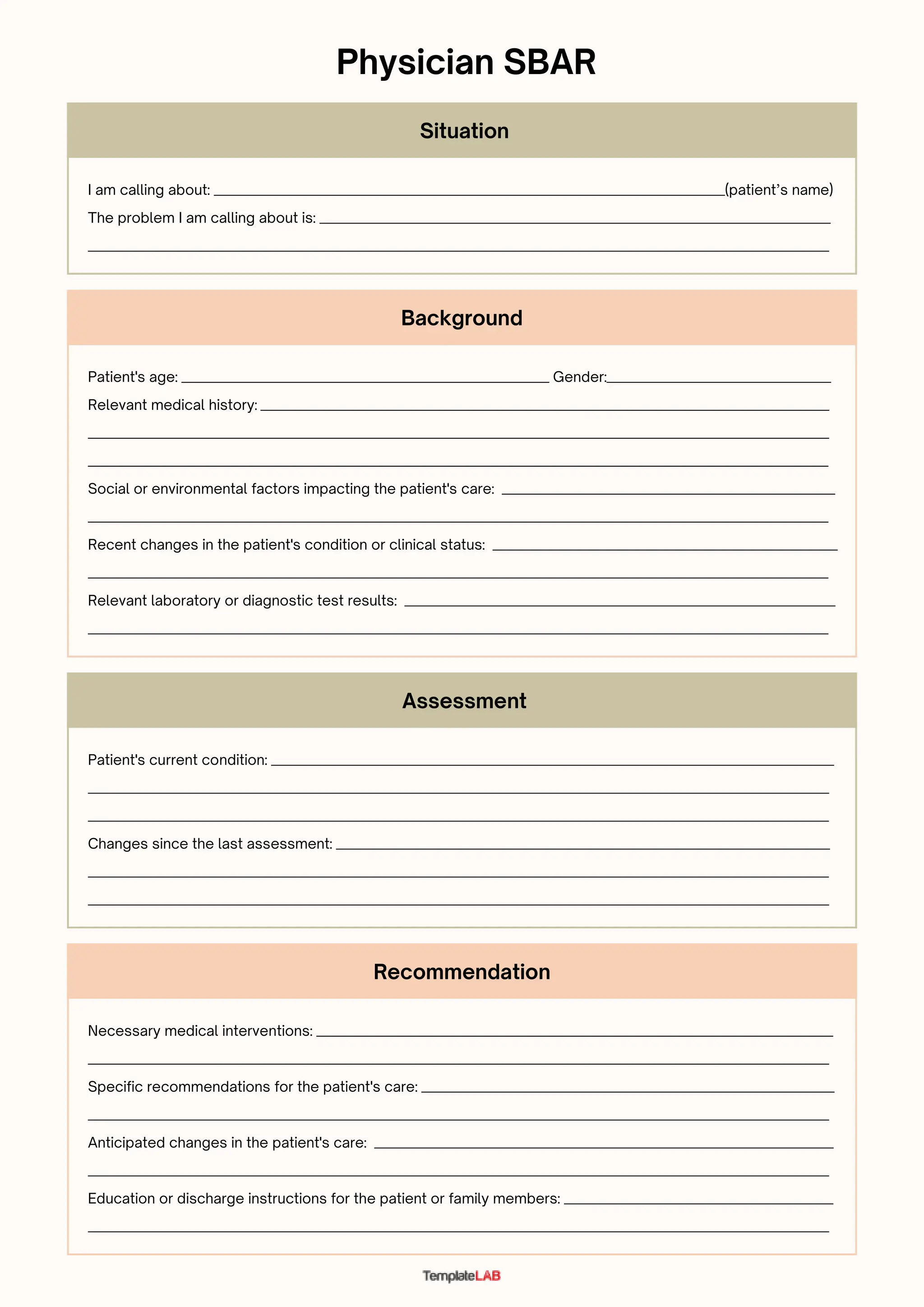
The document provides background information on a patient including their age, gender, medical history, social factors, and recent changes in condition. It also includes a physician SBAR (Situation-Background-Assessment-Recommendation) form which notes the problem being called about, the patient's current condition and any changes, recommendations for necessary interventions and care, anticipated changes, and education or discharge instructions.















![Sbar Pedirevised[1]](https://cdn.slidesharecdn.com/ss_thumbnails/sbarpedirevised1-12801612259946-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



















![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)




