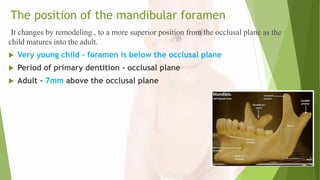
Downloaded 20 times

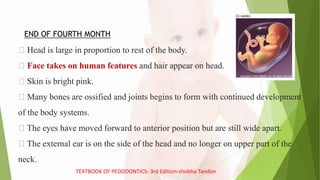


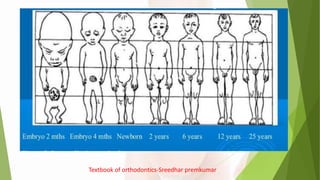
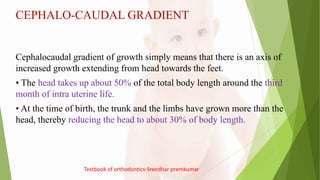
![ The overall pattern of growth continues with a progressive reduction in the relative
size of the head to about 12% in the adult.
The lower limbs are rudimentary around the 2nd month of intrauterine life. They
later grow and represent almost 50% of the body length at adulthood
There is increased gradient of growth evidence even within the head and face
At birth, cranium is proportionally larger than face , Post natally the face grows more
than cranium.
Mandible shows more growth than maxilla post natally
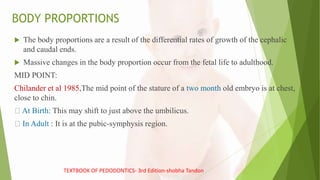
In a new born child the height is measured using measuring tape in a laying position
and referred as LENGTH.[ 40-45 cm]
Textbook of orthodontics-Sreedhar premkumar](https://image.slidesharecdn.com/pedologicanatomynew-190831152206/85/Pedologic-Anatomy-28-320.jpg)



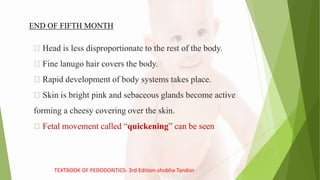
![After birth: Size of cerebral cranium increase by about 50% while the facial skeleton
will grow more than twice the original size.
By 4 years: This growth is completed.
Cranial circumference increase from about 33cm [ birth] - 50cm [at 3 yrs]. After
which it only increase by 6cm.
After 4years onwards : Facial skeleton increases in all direction.
NOTE : Due to above craniofacial changes features of head and face are observed to
be different at different ages
Textbook of human anatomy by BD CHOURASIAS - 7th edition- volume 1](https://image.slidesharecdn.com/pedologicanatomynew-190831152206/85/Pedologic-Anatomy-46-320.jpg)
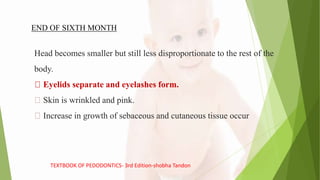
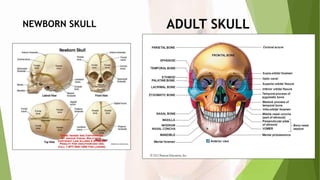
![CLOSURE OF FONTANELLE:
a) Anterior Fontanelle [Frontal] : 18-24 months after birth.
b) Posterior Fontanelle [occipital]: 2 months after birth
c) Antero-lateral Fontanelle [Sphenoid] : 3 months after birth (paired)
d) Postero- lateral Fontanelle [mastoid]: begins to close 1-2 months after birth, closed
completely by 12 months
Textbook of human anatomy by BD CHOURASIAS - 7th edition- volume 1](https://image.slidesharecdn.com/pedologicanatomynew-190831152206/85/Pedologic-Anatomy-51-320.jpg)
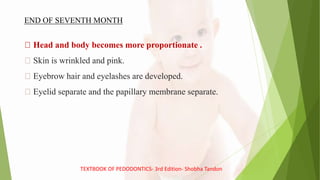
![MANDIBLE
Although still separated by symphysis in the mid-line, the two halves of the mandible fuse
into a single bone by the age of 1-2 yrs.
AT BIRTH:
The two rami are short.
Condylar development is minimal.
A thin line of fibrocartilage and connective tissue exists at the midline of the symphysis
to separate the right and left mandibular bodies.
The symphysial cartilage is replaced by bone [ between 4 months of age –end of the 1
year].
Growth is quite general, with all surface showing bone apposition, especially at the
alveolar border, distal and superior surface of the ramus, condyle, lower border and
lateral surface of the mandible.
Textbook of human anatomy by BD CHOURASIAS - 7th edition- volume 1](https://image.slidesharecdn.com/pedologicanatomynew-190831152206/85/Pedologic-Anatomy-57-320.jpg)
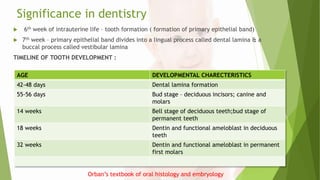
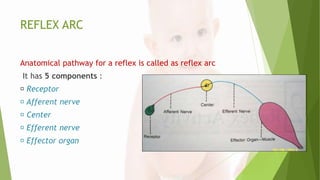
![TEMPEROMANDIBULAR JOINT [TMJ]
The temporomandibular joints (TMJ) are the two
joints connecting the jawbone to the skull.
It is a bilateral synovial articulation between the
temporal bone of the skull above and the mandible
below
STRUCTURE
The main components are the joint capsule, articular
disc, mandibular condyles, articular surface of the
temporal bone, temporomandibular ligament,
stylomandibular ligament, sphenomandibular
ligament, and lateral pterygoid muscle.](https://image.slidesharecdn.com/pedologicanatomynew-190831152206/85/Pedologic-Anatomy-60-320.jpg)



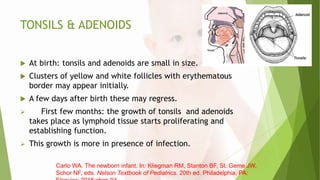
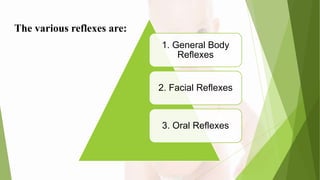
![BUCCAL PAD OF FAT [CORPUS ADIPOSUM /
BICHAT’S FAT PAD]
It is a child reserve of energy.
child cheek prominence giving a chubby appearance.
It is formed of a firm encapsulated mass of fat lying between the
subcutaneous fat and the muscle of the cheek.
Its exact role in suckling is not known.
It probably plays no role in suckling, but it has been found to regress
once suckling has ceased
Carlo WA. The newborn infant. In: Kliegman RM, Stanton BF, St. Geme JW, Schor NF, eds.
Nelson Textbook of Pediatrics. 20th ed. Philadelphia, PA: Elsevier; 2016:chap 94.](https://image.slidesharecdn.com/pedologicanatomynew-190831152206/85/Pedologic-Anatomy-72-320.jpg)








![CONCLUSION
Knowledge of PEDOLOGIC ANATOMY is very helpful to PEDODONTIST as
it not only serves as an adjunct in DIANOSIS but also aids in TREATMENT
PLANNING.
The knowledge of different growth spurts helps in planning treatment especially
in Interceptive Orthodontics where growth can be modified or surgery is
indicated. [ e.g. Cleft lip & Palate]](https://image.slidesharecdn.com/pedologicanatomynew-190831152206/85/Pedologic-Anatomy-121-320.jpg)

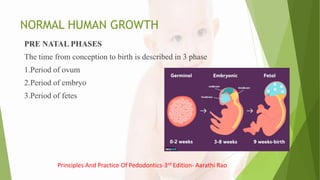
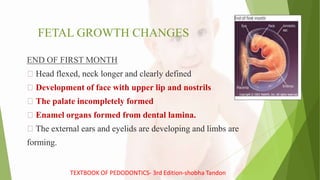
The document discusses pediatric anatomy and growth changes from fetal development through childhood. Key points: 1. Fetal growth occurs in three phases - the period of the ovum, embryo, and fetus. During these phases, major organs develop and body proportions change significantly from the head comprising 50% of body length early in gestation to 30% at birth. 2. Postnatal, general proportions continue changing as the trunk and limbs grow more than the head. The skull and facial bones also change proportions and fuse at different ages. 3. Growth occurs in spurts, with the most significant in early childhood and during adolescence. Girls generally experience growth spurts earlier than boys.



































































