Downloaded 366 times



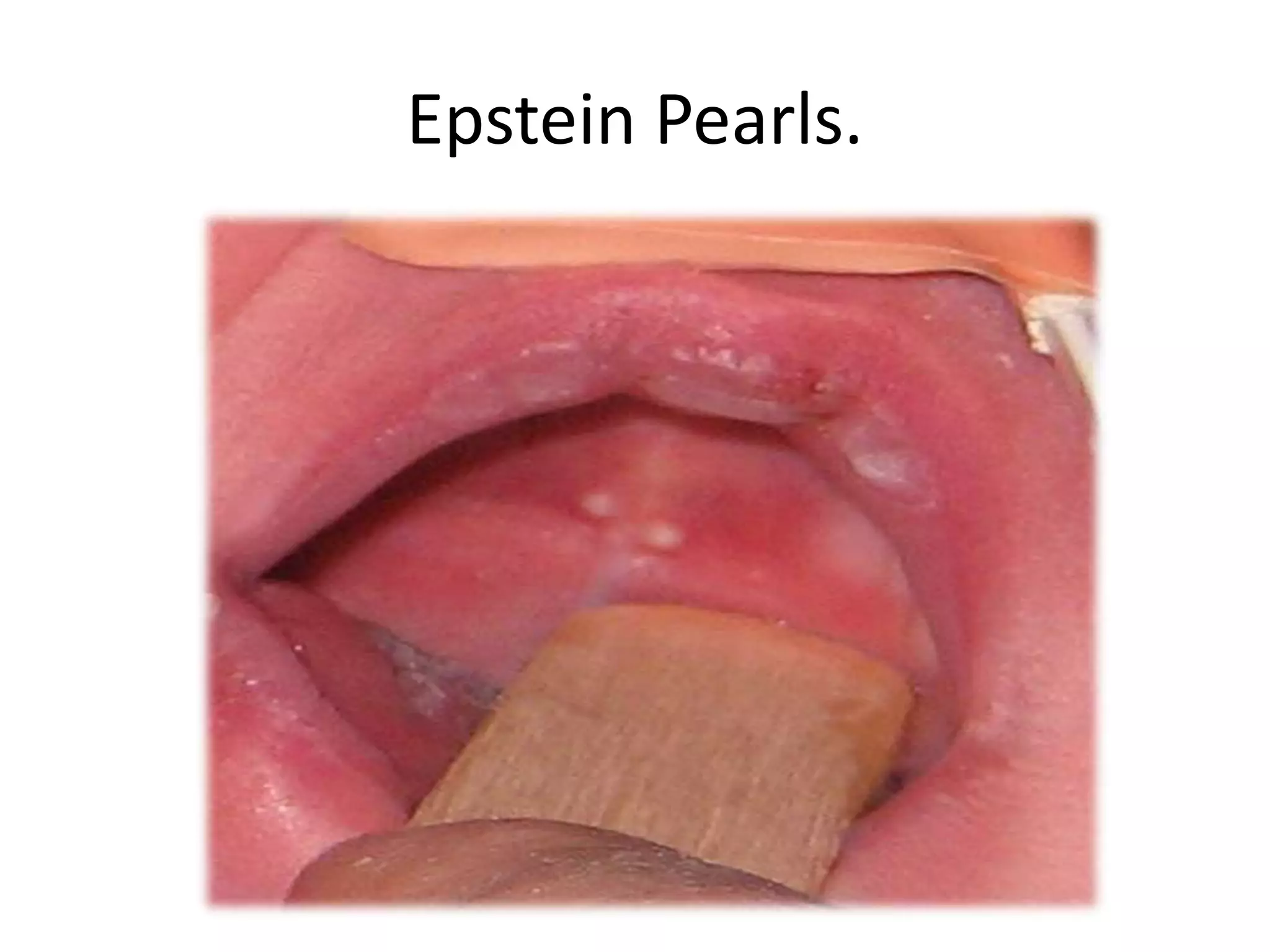


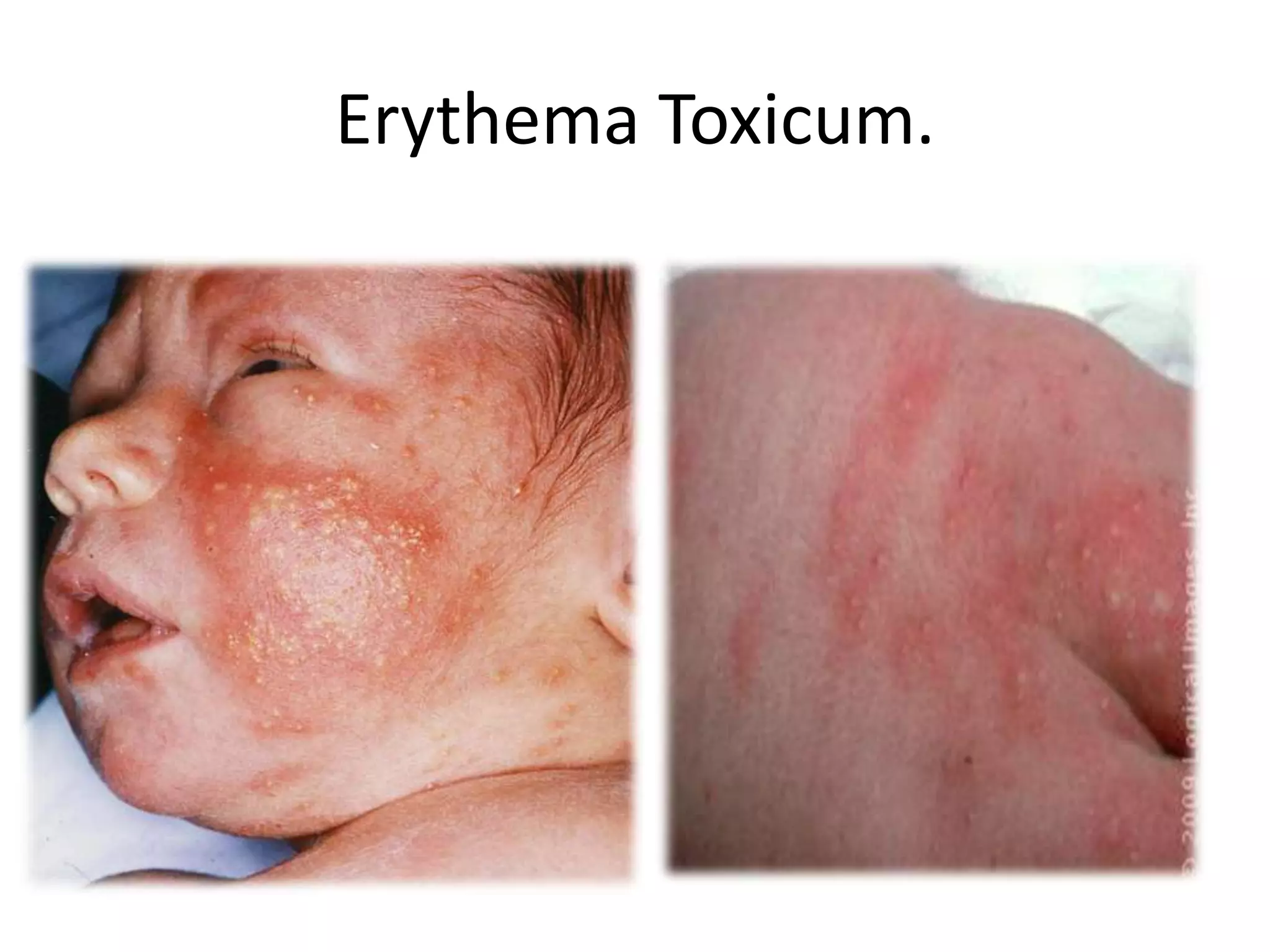




















































This document provides information on several common pediatric dermatologic conditions seen in newborns and children, including: - Epstein pearls, which are cysts that form in the mouth of newborns and disappear within 1-2 weeks. - Stork bites (nevus simplex), a common pink birthmark seen in one third of newborns that usually fades within 18 months. - Erythema toxicum, a self-limiting rash seen in 50% of newborns characterized by small papules. - Milia, tiny white skin-colored bumps on the face of newborns that disappear within weeks without treatment. It







![Approach to a_child_with_rash[1]](https://cdn.slidesharecdn.com/ss_thumbnails/approachtoachildwithrash1-180504150522-thumbnail.jpg?width=640&height=640&fit=bounds)





















![1.1.1. bacterial infection of skin [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/1-1-1-bacterialinfectionofskincompatibilitymode-130325014737-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)













































































