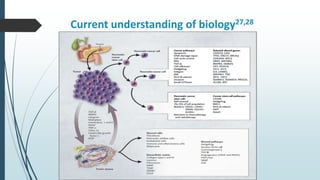
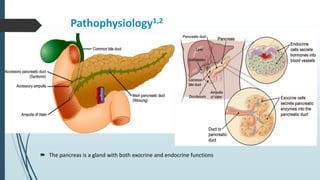
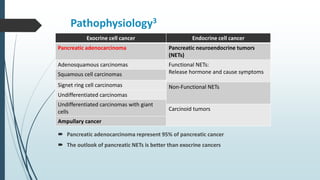
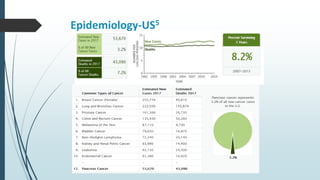
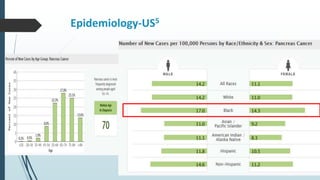
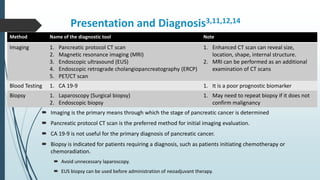
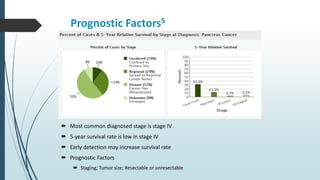
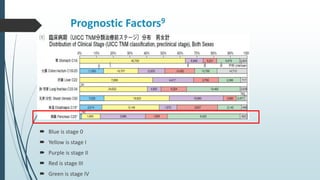
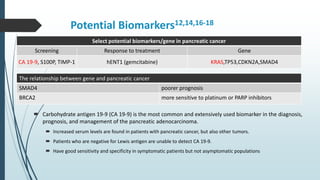
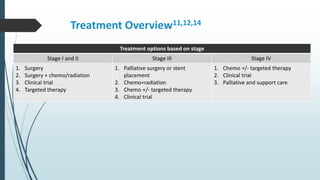
The document provides a comprehensive overview of pancreatic cancer, detailing its pathophysiology, epidemiology, risk factors, and treatment options. It highlights the high mortality associated with the disease, the significance of early diagnosis, and various treatment modalities including surgery, chemotherapy, and investigational therapies. Notably, the text emphasizes the limited survival rates, particularly in advanced stages, and the potential for emerging immunotherapies.





![First line therapy comparison21
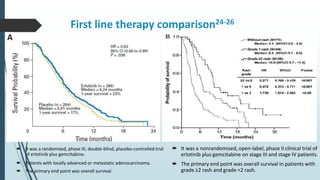
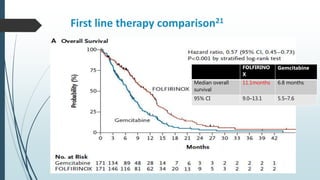
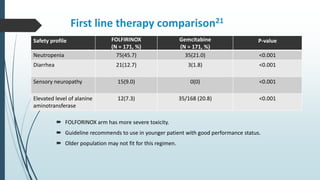
It was a randomized, phase 2–3 trial of receiving FOLFIRINOX or gemcitabine.
Patients with confirmed, measurable metastatic pancreatic adenocarcinoma and treatment-naïve.
The primary end point was overall survival.
FOLFIRINOX
(N = 171)
Gemcitabine
(N = 171)
Objective Response Rate, n (%)
[95% CI]
P value
54 (31.6)
[24.7–39.1]
< 0.001
16 (9.4)
[5–14.7]
—
Response, n (%)
Complete response
Partial response
Stable disease
Progressive disease
Could not be evaluated
1 (0.6)
53 (31.0)
66 (38.6)
26 (15.2)
25 (14.6)
0
16 (9.4)
71 (41.5)
59 (34.5)
25 (14.6)
Rate of disease control, n (%)
[95% CI]
P value
120 (70.2)
[62.7–76.9]
< 0.001
87 (50.9)
[43.1–58.6]
—](https://image.slidesharecdn.com/pancreaticcancerpresentaion-171024180556/85/Pancreatic-cancer-presentaion-33-320.jpg)
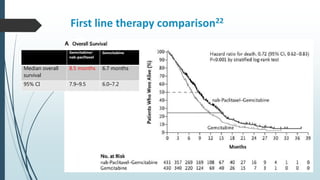
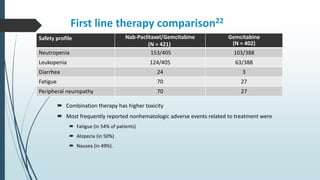
![First line therapy comparison22
It was a randomized, phase 3 trial receiving of Nab-Paclitaxel/gemcitabine or gemcitabine.
Patients with confirmed, measurable metastatic pancreatic adenocarcinoma and treatment-naïve.
The primary end point was overall survival.
Nab-Paclitaxel/Gemcitabine
(N = 431)
Gemcitabine
(N = 430)
Objective Response Rate, n (%)
[95% CI]
P value
99 (23)
[19–27]
< 0.001
31 (7)
[5–10]
—
Response, n (%)
Complete response
Partial response
Stable disease
Progressive disease
Could not be evaluated
1 (<1)
98 (23)
118 (27)
86 (20)
128 (30)
0
31 (7)
122 (28)
110 (26)
167 (39)
Rate of disease control, n (%)
[95% CI]
P value
206 (48)
[43–53]
< 0.001
141 (33)
[28–37]
—](https://image.slidesharecdn.com/pancreaticcancerpresentaion-171024180556/85/Pancreatic-cancer-presentaion-36-320.jpg)